Craig T. Basson, MD, PhD
- Gladys and Roland Harriman Professor of Medicine
- Director, Cardiovascular Research, Cardiology Division
- Weill Medical College of Cornell University
- New York, New York
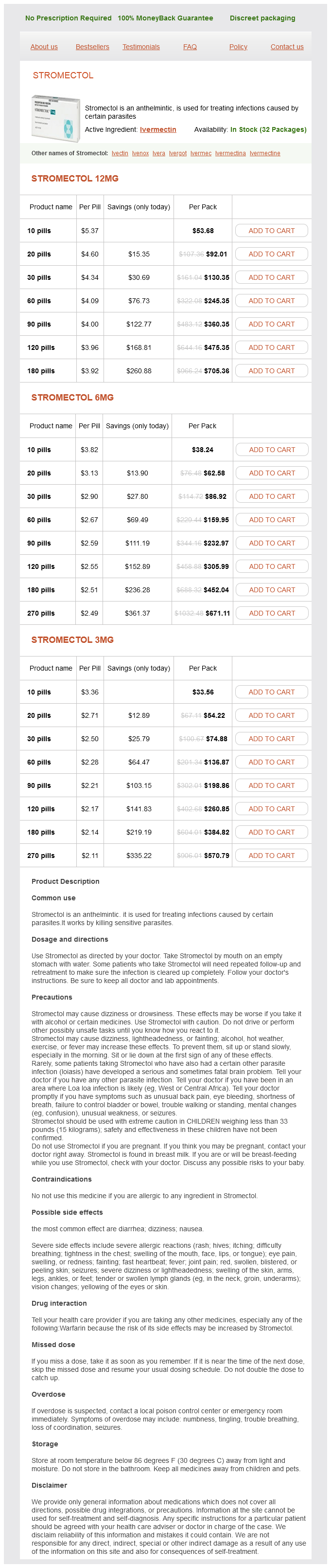
Sulfur mustard gas bacteria weight loss buy simpiox 3 mg cheap, also known as yperite (dichlorodiethyl sulfide) virus 87 simpiox 3 mg buy overnight delivery, has been used in chemical warfare bacteria joe buy simpiox 6 mg. The earliest and most frequently affected sites are areas covered by clothing and humidified by sweat virus x-terminator discount simpiox uk, such as the groin infection urinaire femme cheap simpiox american express, axillae, and genitalia. Otherirritants Metal salts that act as irritants include the cyanides of calcium, copper, mercury, nickel, silver, and zinc and the chlorides of calcium and zinc. Occupational exposure to methyl bromide may produce erythema and vesicles in the axillary and inguinal areas. Insecticides, including 2,2-dichlorovinyl dimethyl phosphate used in roach powder and fly repellents and killers, can act as irritants. Chloracne may persist for long periods because dioxin is stored in the liver and released slowly into the circulation. The irritant properties of petroleum derivatives are directly proportional to their fat-solvent properties and inversely proportional to their viscosity. Oils of the naphthalene series are more irritating than those of the paraffin series. Refined fractions from petroleum are less irritating than the unrefined products, although benzene, naphtha, and carbon disulfide may cause a mild dermatitis. They represent a frequent cause of occupational dermatoses in machine tool operators, machinists, layout men, instrument makers, and setup men. Insoluble (neat) cutting oils are responsible for a follicular acneiform eruption on the dorsa of the hands, the forearms, face, thighs, and back of the neck. Hyperpigmentation, keratoses, and scrotal cancer have been found in those exposed to insoluble cutting oils. Soluble oils and synthetic fluids used in metalworking do not result in acne, but rather an eczematous dermatitis, usually of the dorsal forearms and hands. Allergic contact dermatitis arises from various additives, such as biocides, coloring agents, and deodorizers. Coal briquette makers develop dermatitis as a result of a tarry residue from petroleum used in their trade. Shale oil workers develop an erythematous, follicular eruption that eventually leads to keratoses, which may become the sites of carcinoma. Gradually, keratoses appear, and after many years, some of these are the sites of carcinoma. Melanoderma may occur from exposure to mineral oils and lowergrade petroleum from creosote, asphalt, and other tar products. Petrolatum dermatitis may appear as a verrucous thickening of the skin caused by prolonged contact with impure petroleum jelly or, occasionally, lubricating oil. A follicular-centered process may occur in which erythematous horny nodules are present, usually on the anterior and inner aspects of the thighs. Acne corne consists of follicular keratosis and pigmentation resulting from crude petroleum, tar oils, and paraffin. The dorsal aspects of the fingers and hands, the arms, legs, face, and thorax are the areas usually involved. The lesions are follicular horny papules, often black, and are associated at first with a follicular erythema and later with a dirty brownish or purplish spotty pigmentation, which in severe cases becomes widespread and is especially marked around the genitals. Coal tar and pitch and many of their derivatives produce photosensitization and an acneiform folliculitis of the forearms, legs, face, and scrotum. Mace is a mixture of tear gas (chloroacetophenone) in trichloroethane and various hydrocarbons resembling kerosene. Treatment consists of changing clothes, then washing with oil or milk, followed by washing with copious amounts of water. Chloracne 92 Workers in the manufacture of chlorinated compounds may develop chloracne, with small, straw-colored follicular plugs and papules, chiefly on the malar crescent, retroauricular areas, earlobes, neck, shoulders, and scrotum. Histologically, there is a loss of sebaceous glands and the formation of cystic structures. The synthetic waxes chloronaphthalene and chlorodiphenyl, used in the manufacture of electric insulators and in paints, varnishes, and lacquers, predispose workers engaged in the manufacture of these synthetic waxes to chloracne. Exposure to 2,6-dichlorobenzonitrile during the manufacture of a herbicide, and to 3,4,3,4-tetrachloroazooxybenzene, which is an unwanted intermediate byproduct in the manufacture of a pesticide, may also produce chloracne. A contaminant in the synthesis of herbicides and hexachlorophene, 2,3,7,8-tetracholorodibenzo-p-dioxin, produces a chemical burn in the acute stage, but chloracne, hyperpigmentation, hirsutism, and skin fragility (with or without criteria for porphyria cutanea tarda) are manifestations of chronic toxicity. Gastrointestinal tract cancer and malignancies of the lymphatic and hematopoietic systems are suspected to result. Soot, lamp black, and the ash from peat fires produce dermatitis of a dry, scaly character, which over time forms warty outgrowths and cancer. Acquired perforating disease may occur in oil field workers who use drilling fluid containing calcium chloride. Patients develop tender, umbilicated papules of the forearms that microscopically show transepidermal elimination of calcium. Allergiccontactdermatitis Allergic contact dermatitis results when an allergen comes into contact with previously sensitized skin. Persons may be exposed to allergens for years before finally developing hypersensitivity. Genetic variability in the immunologic processes leading to sensitization and other factors, such as concentration of the allergen applied, its vehicle, timing and site of the exposure, presence of occlusion, age, gender, and race of the patient, and presence of other skin or systemic disorders, likely determine whether any given exposure will result in sensitization. Once sensitized, however, subsequent outbreaks may result from extremely slight exposure. Childhood exposures do result in allergy, and the frequency of allergy in this age group is increasing. Sensitivity is rarely lost over the years; older patients have similar rates of allergy as adults. Occasionally, dermatitis may be induced when the allergen is taken internally by a patient first sensitized by topical application, as with substances such as cinnamon oil or various medications. It may appear first at the site of the prior sensitization or past positive patch test, but may spread to a generalized morbilliform or eczematous eruption. The most common causes of contact dermatitis in the United States are toxicodendrons (poison ivy, oak, or sumac), nickel, balsam of Peru (Myroxylon pereirae), neomycin, fragrance, formaldehyde and the formaldehyde-releasing preservatives, bacitracin, and rubber compounds. Frequent positive reactions to gold and thimerosal do not often correlate with the clinical exposure history. Gold reactions, which may be prolonged, can be correlated in some cases with oral gold exposure or occupational dermatitis, but in most cases, the relevance is questionable. Thimerosal reactions are probably related to its use as a preservative in common vaccines and skin-testing material. Eczematous delayed-type hypersensitivity reaction, as exemplified by allergic contact dermatitis and the patch test, must be distinguished from immediate-type hypersensitivity reaction. The latter presents within minutes of exposure with urticaria and is proved with a scratch test. In some patients, impetigo, pustular folliculitis, and irritation or allergic reactions from applied medications are superimposed on the original dermatitis. A particularly vexing situation is when allergy to topical corticosteroids complicates an eczema, in which case the preexisting dermatitis usually does not flare, but simply does not heal as expected. The cutaneous reaction may also provoke a hypersusceptibility to various other, previously innocuous substances, which continues the eczematous inflammatory response indefinitely. For acute generalized allergic contact dermatitis, treatment with systemic steroidal agents is effective, beginning Solvents the solvents cause approximately 10% of occupational dermatitis. When solvents are applied to the hands to cleanse them, the surface oil is dissolved, and a chronic fissured dermatitis results. Additionally, peripheral neuropathy and chemical lymphangitis may occur after the solvents are absorbed through the fissured skin. Solvent sniffers may develop an eczematous eruption around the mouth and nose; erythema and edema occur. This is a direct irritant dermatitis caused by the inhalation of the solvent placed on a handkerchief. Trichloroethylene is a chlorinated hydrocarbon solvent and degreasing agent also used in the dry-cleaning and refrigeration industry. Inhalation may produce exfoliative erythroderma, mucous membrane erosions, eosinophilia, and hepatitis. Allergic contact dermatitis caused by alcohol is rarely encountered with lower-aliphatic alcohols. A severe case of bullous and hemorrhagic dermatitis on the fingertips and deltoid region was caused by isopropyl alcohol. LandeckL,etal: Clinical course of occupational irritant contact dermatitis of the hands in relation to filaggrin genotype status and atopy. SeyfarthF,etal: Dry skin, barrier function, and irritant contact dermatitis in the elderly. When the eruption is limited in extent and severity, local application of topical corticosteroid creams, lotions, or aerosol sprays is preferred. Testingforsensitivity Patch test the patch test is used to detect hypersensitivity to a substance that is in contact with the skin so that the allergen may be determined and corrective measures taken. So many allergens can cause allergic contact dermatitis that it is impossible to test a person for all of them. In addition, a good history and observation of the pattern of the dermatitis, its localization on the body, and its state of activity are helpful in determining the cause. The patch test is confirmatory and diagnostic, but only within the framework of the history and physical findings; it is rarely helpful if it must stand alone. Interpretation of the relevance of positive tests and the subsequent education of patients are challenging in some cases. The patch test consists of application of substances suspected to be the cause of the dermatitis to intact uninflamed skin. Dermatitis originating in the workplace will almost always require individualized testing. Test substances are applied usually to the upper back, although if only one or two are applied, the upper outer arm may be used. The patches are removed after 48 h (or sooner if severe itching or burning occurs at the site) and read. The patch sites need to be evaluated again at day 4 or 5 because positive reactions may not appear earlier. Some allergens may take up to day 7 to show a reaction, and the patient should be advised to return if such a delayed reaction occurs. Occasionally, patch tests for potassium iodide, nickel, or mercury will produce pustules at the site of the test application. Usually no erythema is produced; therefore, the reaction has no clinical significance. Strong patch test reactions may induce a state of hyperirritability ("excited skin syndrome") in which adjacent tests that would otherwise be negative appear as weakly positive. The oral mucosa is more resistant to primary irritants and is less liable to be involved in allergic reactions. This may be because the keratin layer of the skin more readily combines with haptens to form allergens. Also, the oral mucosa is bathed in saliva, which cleanses and buffers the area and dilutes irritants. However, patch testing for various types of oral signs and symptoms, such as swelling, tingling and burning, perioral dermatitis, and the appearance of oral lichen planus, is useful in determining a cause in many cases. False-negative reactions may result; the value of testing in such circumstances is that if a positive reaction occurs, a diagnosis may be made. Provocative use test the provocative use test will confirm a positive closed patch test reaction to ingredients of a substance, such as a cosmetic; it is used to test products that are made to stay on the skin once applied. The material is rubbed on to normal skin of the inner aspect of the forearm several times a day for 5 days. To test for 6-methyl coumarin sensitivity, the patch is applied in the same manner but for only 30 min before light exposure, rather than for 48 h. A duplicate set of nonirradiated patches is used in testing for the presence of routine delayed hypersensitivity reactions. There is a steady increase in incidence of photoallergy to sunscreening agents and a decreasing incidence of such reactions to fragrance. Regionalpredilection Familiarity with certain contactants and the typical dermatitis they elicit on specific parts of the body will assist in diagnosis of the etiologic agent. Head and neck the scalp is relatively resistant to the development of contact allergies; however, involvement may be caused by hair dye, hair spray, shampoo, or permanent wave solutions. The metallic rivets in blue jeans may lead to periumbilical dermatitis in nickel-sensitive patients, as may piercings of the umbilicus. The groin is usually spared, but the buttocks and upper thighs may be sites of dermatitis caused by dyes. The perianal region may be involved from the "caine" medications in suppositories, as well as preservatives and fragrances in cleansing materials. Almost half of women with pruritus vulvae have one or more relevant allergens; often these are medicaments, fragrances, or preservatives. Persistent otitis of the ear canal may be caused by sensitivity to neomycin, an ingredient of most aural medications. Volatile gases, false-eyelash adhesive, fragrances, preservatives, mascara, rubber in sponges used to apply cosmetics, and eyeshadow are also frequently implicated. Perioral dermatitis and cheilitis may be caused by flavoring agents in dentifrices and gum, as well as fragrances, shellac, medicaments, and sunscreens in lipstick and lip balms. There is a typical clear area under the chin where there is little or no exposure to sunlight. The left cheek and left side of the neck (from sun exposure while driving) may be the first areas involved. Feet are sites for shoe dermatitis, most often attributable to rubber sensitivity, chrome-tanned leather, dyes, or adhesives. Application of topical antibiotics to stasis ulcers frequently leads to sensitivity and allergic contact dermatitis. Trunk the trunk is an infrequent site; however, the dye or finish of clothing may cause dermatitis.
Promising pharmacological antibiotic resistance news headlines buy cheap simpiox on-line, molecular and cellular treatments of autoimmune hepatitis treatment for dogs eating poop generic simpiox 12 mg buy line. Review article: the management of autoimmune hepatitis beyond consensus guidelines antimicrobial vs antibacterial 3 mg simpiox purchase visa. Features associated with treatment failure in type 1 autoimmune hepatitis and predictive value of the model of end stage liver disease bacteria kit generic simpiox 12 mg line. Early predictors of corticosteroid treatment failure in icteric presentations of autoimmune hepatitis antibiotic vs antimicrobial purchase simpiox 6 mg with visa. Despite an increasing frequency of asymptomatic or subclinical disease, greater than 40% affected patients with either condition generally present with the gradual onset of fatigue and pruritus. Fatigue can be problematic, and it is important to evaluate for other causes of this symptom such as medication side effects, hypothyroidism, or depression. However, other etiologic factors of malabsorption can include pancreatic exocrine insufficiency, coexisting celiac disease, or bacterial overgrowth. A history of previous reconstructive biliary surgery, the presence of dominant extrahepatic biliary strictures, or the development of a superimposed cholangiocarcinoma may also be responsible. The symptoms of end-stage liver disease, such as gastrointestinal bleeding, ascites, and encephalopathy, occur late in the course of both diseases. Physical examination may reveal jaundice and excoriations from pruritus in both disorders. The spleen may also be palpable if portal hypertension from advanced disease has developed. Characteristics of end-stage liver disease, including muscle wasting and spider angiomata, appear in the advanced stages of both diseases. Anti-M8, when present with anti-M2, may be associated with a more rapid course of disease progression in selected patients. Magnetic resonance cholangiogram exhibiting classic features of primary sclerosing cholangitis, including diffuse intrahepatic stricturing and dilation. Florid duct lesion (granulomatous bile duct destruction) in primary biliary cirrhosis. A poorly formed granuloma surrounds and destroys the bile duct in an eccentric fashion. The interlobular bile duct shows a typical fibrous collar, and the epithelium seems undamaged. Estimates of overall median survival without liver transplantation range between 10 and 12 years from the time of diagnosis; advanced histologic disease imparts a median survival approaching 8 years. Indeed, nearly a quarter of patients who were asymptomatic at the time of diagnosis will develop clinical symptoms after 5 years. They are useful for developing endpoints of treatment failure and designing therapeutic trials. Several studies have suggested that improvements in serum alkaline phosphatase over time are associated with improved outcomes. For example, the persistent improvement of alkaline phosphatase to less than or equal to 1. The occurrence of diminished visual acuity at night can be attributed to vitamin A deficiency. Vitamin D deficiency occurs commonly in association with marked steatorrhea, which is related to a decrease in small bowel bile acid concentration. Other factors that may contribute to malabsorption can include pancreatic insufficiency, bacterial overgrowth, or celiac disease. Finally, vitamin E deficiency infrequently occurs, but when present results in neurologic abnormalities affecting the posterior spinal columns, leading to areflexia, loss of proprioception, and ataxia. Risk factors for osteoporosis include advancing age, low body mass index, previous history of fractures, and advanced histologic disease. Both vitamin D deficiency and smoking have been implicated as risk factors for metabolic bone disease. Additional risk factors that have been described in the general population include glucocorticoid use, excessive alcohol intake, smoking, or having a parent who sustained a fracture. This is typically after endoscopic biliary manipulation (rare in era of prophylactic antibiotics) or secondary to obstructing strictures, malignancy, or stones. When encountered, it should immediately raise a suspicion for the presence of cholangiocarcinoma. When encountered, fluorescence in situ hybridization may detect chromosomal abnormalities (such as polysomy) from biliary brushings and can aid in the diagnosis of cholangiocarcinoma. Nearly one quarter of cases are diagnosed either at the time of diagnosis or within the first 2 years after patients present. However, individuals with cirrhosis should be enrolled in a 6-month, ultrasound-based screening program. Importantly, colorectal neoplasia can develop soon after the two conditions are diagnosed. The presence of a mass lesion with delayed venous enhancement is indicative of cholangiocarcinoma. The presence of chromosomal polysomy detected by fluorescence in situ hybridization should also raise concern for cholangiocarcinoma. Drug-induced cholestasis secondary to phenothiazines, estrogens, azoles, and a number of other drugs also should be considered as alternative diagnoses. If the cholangiogram is normal, patients should have a liver biopsy to establish the diagnosis. Lymphocytic piecemeal necrosis and coexistent portal inflammation with bile duct destruction are commonly seen. In addition, it increases the intestinal excretion of bile acids by preventing their absorption. It is administered in 4-g doses (mixed with liquids) with meals or after breakfast for a total daily dose of 12 to 16 g. Once the itching remits, the dosage should be reduced to the minimal amount that maintains relief. Rifampin at a dosage of 300 to 600 mg/day also has been effective in relieving pruritus caused by either p450 enzyme induction or inhibition of bile acid uptake. Anecdotal benefit with gabapentin has been reported and may be helpful when liver dysfunction precludes the safe use of rifampin. For refractory cases, sertraline 100 mg a day or naltrexone 50 mg a day could be considered. In the setting of dominant strictures, endoscopic decompression may improve cholestasis and alleviate pruritus. Intractable pruritus is an indication for liver transplantation, which results in symptomatic relief. Treatment of osteoporosis includes exercise, adequate supplementation of calcium and vitamin D, and a bisphosphonate. Bisphosphonates are considered a first-line agent for the treatment of osteoporosis. For individuals with esophageal varices, a parenteral bisphosphonate should be used. Problems with night vision caused by vitamin A deficiency may be alleviated by oral replacement therapy. Decreased serum levels can be corrected with the oral administration of vitamin A (25,000 to 50,000 units) two or three times per week. Because excessive vitamin A intake has been associated with hepatotoxicity, serum levels should be frequently monitored. In patients with low vitamin E levels, oral replacement therapy with 400 units/day can be instituted. The administration of ciprofloxacin results in high biliary concentrations and has broad gram-negative and gram-positive coverage. Similar results can be observed with other fluoroquinolones, such as norfloxacin and levofloxacin. Prophylactic therapy with oral fluoroquinolone therapy may reduce the frequency of recurrent cholangitis, although no controlled trial has been performed to support this conclusion. Balloon dilation is most effective in patients with acute elevations of serum total bilirubin level or recent onset of bacterial cholangitis. It appears less effective in patients with long-standing jaundice or a history of recurrent bacterial cholangitis. Although some studies have suggested an increased risk of complications following biliary stenting, this finding has not been consistently observed. Therefore temporary biliary stents should be used for strictures refractory to balloon dilation. A short course (57 days) of oral antibiotics following dilation or stenting can reduce the risk of postprocedural cholangitis as well. For strictures related to cholangiocarcinoma, the use of expandable metal stents can be employed for palliative treatment. Pharmacologic agents such as colchicine, corticosteroids, cyclosporine, azathioprine, methotrexate, and mycophenolate mofetil have demonstrated marginal clinical benefit and significant adverse effects. For example, men are less likely to respond than women (72% versus 80%, respectively). In addition, those who present at an older age (older than 70 years) have a response rate of 90% compared with a response rate of 50% among patients who were diagnosed at a younger age (younger than 30 years). Factors that influence the consideration for liver transplantation are deteriorating hepatic synthetic function, the development of comorbid conditions. However, recurrent cholangitis has not been associated with an increase in wait-list mortality. No significant effect on survival, however, has been associated with recurrent histologic disease. Tacrolimus-based immunosuppression is associated with a shorter time-to-recurrence than cyclosporine-based therapy. A mesenteric defect can be created during the biliary reconstruction which is typically a Roux-en-Y choledochojejunostomy. The epidemiology and natural history of primary biliary cirrhosis: a nationwide population-based study. Population-based epidemiology, malignancy risk and outcome of primary sclerosing cholangitis. Pathogenesis of primary sclerosing cholangitis and advances in diagnosis and management. Long-term effects of mid-dose ursodeoxycholic acid in primary biliary cirrhosis: a meta-analysis of randomized controlled trials. This in turn causes an immunologic response through the generation of memory B cells that produce antibodies, which provide varying protection from the pathogen in the future. Immunizations allow for the controlled exposure to pathogens or proteins that induce these protective antibody responses, and have helped control the spread of infectious diseases significantly since their introduction. Inactivated vaccines, also known as killed vaccines are those in which the pathogen stimulates antibody production by triggering an immunologic response. Attenuated vaccines, also known as live vaccines, are made from pathogens that have been disabled from causing active disease. They are still able to stimulate antibody production resulting in protection from the disease, but in patients with compromised immunity this may theoretically result in infection with the pathogen being introduced in the vaccine. How long after receiving the hepatitis A vaccine does it take before one is considered protected against infection There is some evidence of protection in certain individuals within 2 to 4 weeks, but currently 4 weeks is the timeframe recommended before someone can be considered to be protected from hepatitis A. Protection after vaccination has been estimated to last 25 years in those vaccinated as adults and up to 20 years in those vaccinated as children. It has been found to be as effective as Ig, which was previously the only recommended way to protect individuals exposed to hepatitis A prior to 2007. Common sense dictates that the following individuals should not be vaccinated: · Individuals who are moderately or severely ill · Individuals allergic to any component of the vaccine or who have previously had a serious allergic reaction to the vaccine 10. The most common recommendation is to give a three-dose series of hepatitis B vaccine. Give the second dose 1 month after the first dose, and give the third dose approximately 5 months after the second. If there is an interruption between doses of hepatitis B vaccine, does the vaccine series need to be restarted If the vaccine series was interrupted after the first dose, the second dose should be administered as soon as possible. The second and third doses should be separated by an interval of at least 8 weeks. For a person with a normal immune system who has received previous vaccination, booster doses are not recommended. The liver plays a key role within the innate immune response because it encounters ingested pathogens from the gut via circulation from the portal vein system. Cirrhotic patients have a fibrotic and poorly functioning liver with dysfunction of the reticuloendothelial system (Kupffer cells in the liver, macrophages, and monocytes) as well as granulocytes (neutrophils, eosinophils, and basophils). There have been studies demonstrating increased gut permeability of bacteria and associated toxins in patients with cirrhosis leading to spontaneous infections. There is frequently extensive shunting of venous circulation away from the liver in patients with cirrhosis, thus impairing clearing capacity following infections. What vaccine-preventable bacterial infections pose an increased risk for patients with cirrhosis Why is vaccination against hepatitis A and B strongly recommended in patients with cirrhosis When should vaccinations against hepatitis A and B be given to cirrhotic patients For both hepatitis A and B it is recommended that vaccinations be given early in the disease course. Patients have a better immune response to the vaccines when they are given shortly after developing cirrhosis when compared with those who receive it in the later stages of their disease. The patients should receive the standard two doses of the hepatitis A vaccine and three doses of the hepatitis B vaccine per normal guidelines if in the early stages of chronic liver disease, although patients with more advanced disease. Furthermore, studies have demonstrated increased hepatic decompensation in patients with advanced cirrhosis who develop influenza infections. Patients with cirrhosis should receive the pneumococcus vaccine as close as possible to the time of diagnosis, regardless of age. In addition to individuals older than 65 years, pneumococcal infections are more prevalent in patients with cirrhosis and others with chronic liver disease. In patients with concurrent alcoholism and liver cirrhosis, their risk of death from pneumococcal pneumonia, meningitis, or bacteremia is greatly increased.
So antibiotics for uti uk buy 6 mg simpiox with visa, ideally bacteria for septic tanks purchase cheap simpiox on-line, two biopsy samples are sent-one in formalin and another fresh for freezing antibiotics in the sun simpiox 3 mg order amex. Also antibiotics for acne side effects 12 mg simpiox buy with visa, submucosa should be included in the biopsy samples to assess nerves in both the lamina propria and muscularis mucosae antimicrobial beer line simpiox 12 mg purchase on line. The high-grade lesions are associated with high-risk human papillomavirus 16 and 18, among others. What are the cells of origin and the immunohistochemical profile of Paget disease The Paget cells (intraepithelial large cells with pale pink cytoplasm and large nuclei) are believed to be of apocrine lineage and show immunoreactivity with low-molecular-weight keratins Cam 5. Pathology features in Bethesda guidelines predict colorectal cancer microsatellite instability: A population-based study. Serrated polyps of the large intestine: A morphologic and molecular review of an evolving concept. A histopathologic study of gastric and small intestinal graft-versus-host disease following allogenic bone marrow transplantation. Eighty percent of foreign-body ingestions occur in children, whereas almost all foreign bodies inserted into the rectum are described in adults. Groups at increased risk for foreign-body ingestion include psychiatric patients, prisoners, and those who frequently and excessively use alcohol or sedative-hypnotic medications. Also at risk are older adult subjects, who may have poorly fitting dentures, impaired cognitive function resulting from medications, or dementia or dysphagia after stroke. Intentional ingestion of foreign objects is well described in smugglers of illicit drugs, jewelry, or other valuable items. In addition, numerous pathologic abnormalities, such as strictures or tumors, may impair spontaneous passage of foreign bodies (see Question 12). Accidental loss of sex stimulant devices account for more than one half of foreign objects introduced through the anus. A, Meat bolus (3 Â 1 cm) impacted in the mid esophagus of a patient with diffuse esophageal spasm. B, Inadvertently swallowed partial denture (3 Â 2 cm), with exposed hooks, in the esophagus of a patient without underlying esophageal pathologic findings. C, Dried apricot (2 Â 2 cm) in the colon of a patient with intermittent abdominal pain. D, Chicken bolus (2 Â 2 cm) impacted in distal esophagus of a patient with underlying eosinophilic esophagitis. Adults trace the onset of symptoms to the ingestion of a specific meal or foreign body. Most commonly, acute dysphagia, odynophagia, and chest pain reflect underlying esophageal obstruction. Respiratory distress, stridor, and inability to handle oral secretions suggest the need for urgent intervention. Persons with developmental disabilities, psychiatric patients, or children may remain asymptomatic for months after ingestion, or they may not volunteer the history. Patients with impacted anorectal foreign bodies may relate a wide variety of medical histories to account for their predicament, ranging from accidents or assault to medical remedies. Patients with wheezing, stridor, cough, or dyspnea after foreign-body ingestion may have foreign-body entrapment in the hypopharynx, trachea, pyriform sinus, or Zenker diverticulum. On rare occasions, sharp objects, such as pins, needles, nails, and toothpicks, may perforate the intestine, but in 70% to 90% of cases they pass through the alimentary tract without complication. Two phenomena in the intestine allow safe passage: (1) foreign bodies pass with axial flow down the lumen, and (2) reflex relaxation and slowing of peristalsis cause sharp objects to turn around in the lumen so that the sharp end trails down the intestine. In the colon, the foreign object is centered in the fecal bolus, which further protects the bowel wall. Button alkaline batteries may cause coagulation necrosis in the esophagus, but once they reach the stomach, gastric acid neutralizes their risk. There is no known absolute size of a foreign body that dictates surgical intervention because the shape, composition, and sharpness of edges may play a key role. In general, inert, blunt objects measuring 3 Â 3 cm pass through the intestine, whereas objects longer than 6 cm may become lodged in the C-loop of the duodenum. Ingested magnets from magnetic toy sets may be attracted to one another across multiple loops of bowel and lead to intestinal perforation caused by bowel wall erosion and necrosis between the magnets. Button batteries or magnets, ingested typically by small children, need to be removed urgently because of the severe trauma that they may cause in the esophagus. Any sharp object that carries a high risk for perforation should be removed as soon as possible before it passes to a level that is beyond the reach of an endoscope. For the same reasons, long objects (larger than 6 cm) should be removed when identified. Finally, objects lodged in the esophagus that compromise ability to handle oral secretions should be removed urgently to reduce the risk of aspiration. Describe the signs and symptoms of a complication related to foreign-body ingestion. Respiratory symptoms suggest entrapment of the foreign body in the hypopharynx, trachea, pyriform sinus, or Zenker diverticulum (see Question 6). Sharp objects may penetrate, obstruct, or perforate the esophagus or intestine, presenting with chest, neck, or abdominal pain that varies from mild discomfort to symptoms and signs of acute abdomen. Injury to the esophagus can lead to hematemesis, fever, tachycardia, neck swelling, and crepitus. Excessive drooling and inability to swallow saliva suggest complete esophageal obstruction. Abdominal distention, vomiting, and hyperactive bowel sounds suggest intestinal obstruction. Hypoactive or absent bowel sounds, guarding, rebound, and abdominal pain are seen with wall penetration or free perforation. Aortoenteric fistula caused by ingestion of a sharp foreign body may cause massive hematemesis. Other modalities have been used with variable success, although major complications have been reported. Prior to endoscopy, a rehearsal of what will be done using retrieval devices that would capture similar-shaped foreign objects is useful. Protection of the airway, especially in children or combative or older adult patients with poor reflexes and cardiopulmonary reserve, is essential. Consultation with a surgeon is appropriate for cases in which perforation or other major complications are probable. Combined endoscopic and laparoscopic removal of ingested large foreign bodies: Case report and decisional algorithm. Endoscopic techniques and management of foreign body ingestion and food bolus impaction in the upper gastrointestinal tract: A retrospective analysis of 139 cases. Glucagon use for esophageal coin dislodgment in children: A prospective, double-blind, placebo-controlled trial. Endoscopic management of foreign bodies in the upper gastrointestinal tract: Report on a series of 414 adult patients. In contrast, in the general population, the female-to-male ratio is approximately 1. Thus not only do women have symptoms more frequently than men, but they are also more likely to seek medical attention for their symptoms. The most commonly implicated foods are milk and dairy products, wheat products, onions, peas and beans, hot spices, cabbage, certain meats, smoked products, fried food, and caffeine. They include fructose, lactose, fructans, galactans, and sugar alcohols, such as sorbitol, maltitol, mannitol, xylitol, and ismalt. Fructose and lactose are present in apples, pears, watermelon, honey, fruit juices, dried fruits, milk, and dairy products. Galactans and fructans are present in common dietary constituents, such as wheat, rye, garlic, onions, legumes, cabbage, artichokes, leeks, asparagus, lentils, inulin, soy, Brussels sprouts, and broccoli. However, researchers now believe that noxious stimuli can change the synaptic efficiency of peripheral and central neurons. Through a process known as the wind-up, neurons can develop a pain memory that can persist long after the noxious stimulus is removed. Other symptoms that are common but not essential for the diagnosis include bloating or feeling of abdominal distention, urgency, and incomplete evacuation. A colonoscopy is routinely recommended only in patients older than 50 years of age as per the colon cancer screening guidelines. A colonoscopy for those younger than 50 years of age may be appropriate in patients with significant diarrhea or refractory symptoms or if other alarm features are present (see Question 20). Alarm features such as rectal bleeding, unintended weight loss, fever, age greater than 50 years, nocturnal awakening from sleep, or a family history of colon cancer or inflammatory bowel disease may suggest the presence of an organic disease. Fructose is the sweetest of the sugars and therefore is commonly used as a sweetener in soft drinks, chocolate, syrups, and jams. Up to one half of healthy adults have evidence of malabsorption after ingesting 25 g of fructose (10% concentration). Nevertheless, because of the similarity in symptoms, patients with symptoms suggestive of lactose malabsorption should be given an empiric trial of a lactose-free diet or a lactose hydrogen breath test, which measures the exhaled hydrogen produced from colonic bacterial degradation of lactose. Patients who respond to a lactose-free diet should be encouraged to gradually reintroduce lactose into their diet to determine if and when symptoms recur. Avoidance of lactose can lead to significant reduction in calcium intake, which may increase the risk of osteoporosis. Therefore patients on a restricted lactose diet should be advised to increase their calcium intake from other sources. Live-culture yogurt is another alternative source of calcium that is well tolerated by many patients with lactose intolerance. It is recommended by the American College of Gastroenterology Task Force that serologic testing for celiac disease. If unsuccessful, pharmacologic treatments based on the predominant symptom and severity should be considered. Most patients report that certain foods exacerbate their symptoms and some have adopted an inappropriately restrictive diet. If a correlation exists, the offending food should be eliminated from the diet to discover if symptoms resolve. Excessive air swallowing, which commonly occurs in people who smoke, chew gum, or eat rapidly, may help explain excessive flatulence. Diets consisting of large fatty meals or caffeine may help explain postprandial rectal urgency and bowel frequency. Physical activity has been shown to have a number of positive physiologic and psychological effects. Their overall quality of life scores did not improve, although their physical and cognitive skills did improve. Pharmacologic treatment options for patients who report diarrhea as their predominant symptom include antidiarrheals, such as loperamide, diphenoxylate, cholestyramine, or alosetron. For patients who report constipation as their predominant symptom, treatment options include fiber, osmotic laxatives. For patients who report pain as the predominant symptom, treatment options include antispasmodics. By binding to the opioid receptors on the myenteric neurons in the upper and lower bowel, loperamide reduces gut motility, which allows for greater fluid absorption and improved stool consistency. Loperamide does not cross the blood-brain barrier at standard doses, and therefore does not have central nervous system side effects, such as sedation or addiction. Loperamide 2 to 4 mg each morning after the initial bowel movement and before social events can reduce undesirable urges to defecate, and increases confidence and willingness to engage in social activities. However, in the largest published randomized, placebo-controlled trial to date, desipramine (escalating dose from 50 to 150 mg) was not superior to placebo in intention-to-treat analyses but in a per protocol analysis limited to patients with detectable plasma levels of desipramine showed a significant benefit over placebo. These effects appear to be mostly limited to improvement in well-being and less so in abdominal pain. Antispasmodics can be classified into three major subclasses: anticholinergics, direct smooth muscle relaxants, and peppermint oil. Anticholinergics work by blocking the acetylcholine mediated depolarization of intestinal smooth muscles. In the United States, the most commonly used anticholinergics are dicyclomine and hyoscyamine. Hyoscyamine and dicyclomine can be taken at regular intervals (four times daily) or intermittently for more episodic symptoms. For patients with postprandial symptoms, the medications can be taken 30 to 45 minutes before a meal. For patients with less predictable and more intermittent symptoms, hyoscyamine is preferable because it also comes in an easily dissolvable tablet, which can be taken sublingually and acts within minutes. Hyoscyamine is also available in combination with phenobarbital, scopolamine, and atropine. Although popular, these combination drugs have not been well evaluated in clinical trials and are probably best avoided because of their sedative and addictive potential. Peppermint oil blocks entry of calcium into smooth muscle cells, whereas direct smooth muscle relaxants directly inhibit smooth muscle contractibility by increasing cyclic adenosine monophosphate levels or by interfering with the intracellular calcium pool. Rifaximin is a minimally absorbed oral antibiotic with a broad spectrum of activity and a favorable tolerability profile. Patients receiving rifaximin continue to report improvement in global symptoms after the treatment period as compared with placebo, although its efficacy declines over time. Probiotics are live organisms (bacteria) that are thought to exert a health benefit on the host. Probiotics exert their beneficial effects via several proposed mechanisms including modulation of bacterial flora, improvement of the barrier function of the epithelium, and alteration of the immune activity of the host. There was also significant decrease in abdominal pain and discomfort, bloating, and distention, as well as bowel function.
In sacral fractures allegedly associated with neurologic complications antibiotics for dogs after dog bite cheap simpiox online american express, experience has demonstrated that early traction antibiotic 200 mg discount simpiox 6 mg on line, limiting the rise of the hip bone and the lateral fragment of the aileron antimicrobial zone of inhibition evaluation discount simpiox 12 mg buy, reduces the compression antibiotics have no effect on quizlet cheap simpiox 6 mg visa, which treatment for uti resistant to cipro trusted simpiox 3 mg, together with surgical realignment, favors neurologic recovery. If the clinical examination raises the suspicion of a posttraumatic injury of the lumbosacral plexus, the patient should undergo electrodiagnostic and neuroradiological studies to assess the extent and severity of the nerve damage. The main purpose of these examinations is to determine the presence of root avulsions: preganglionic injuries cannot recover spontaneously. Information given by such techniques is anyway inferred and not directly demonstrated; thus, imaging is actually the core of the diagnostic assessment. But it must be emphasized that the absence of pseudomeningocels does not exclude avulsions and viceversa (intact roots have been visualized inside meningoceles), yet it must be emphasized that these bulky, mushroom-shaped images consequent to the dural tear occurring when the roots are violently pulled out from the spinal cord are still fundamental in the diagnostic assessment of plexal injuries. Therefore, neuroradiological studies also should be performed at least 3 weeks after the trauma, due to the fact that pseudomeningoceles need a few weeks to form. It can also give information on the muscle denervation in correlation with the signal intensity. L5 and S1 are the most frequently avulsed roots; L3 and L4 avulsions are less common and the upper roots are never found avulsed. Once the diagnostic assessment is completed, patients should be referred to a peripheral nerve surgeon, who will ultimately determine whether the injury is amenable to spontaneous recovery or requires surgical treatment. Regardless of the indications for surgery or conservative treatment, patients should start rehabilitation as soon as possible. Intensive physiotherapy is absolutely mandatory to prevent muscle degeneration and joint stiffness with further worsening of the initial clinical picture. A multidisciplinary approach is necessary to obtain adequate pain control, including medical therapy, physical treatments. The patient had previously undergone iliosacral screwing 137 Trauma to the Lumbosacral Plexus 879. Tricyclic antidepressants, opiates, and more recently pregabalin (which has almost completely replaced gabapentin) and tapentadol are the medications more frequently prescribed (often in combination) for the treatment of neuropathic/deafferentation pain. It has been largely demonstrated that reintegrating the patient as soon as possible into an active life, both socially and professionally, has a positive effect on pain control. Mirror visual feedback treatment gives favorable results in chronic pain of central origin, and could possibly be applied in these cases, although no such use has been reported. Nevertheless, it must be acknowledged that in severe deafferentation pain only some degree of symptom control is possible, and in some cases treatment is ineffective; in such cases, surgical options. Some of the recovery is likely to occur as collateral sprouting from healthy or less severely injured neighboring nerves. Anatomical variations of the lumbar plexus: a descriptive anatomy study with proposed clinical implications. Traumatic intradural lumbar nerve root avulsion with associated traction injury to the common peroneal nerve. Am J Roentgenol Radium Ther Nucl Med 1960;84:952957 Tonetti J, Cazal C, Eid A, et al. In lumbosacral plexus injuries can we identify indicators that predict spontaneous recovery or the need for surgical treatment Lumbar plexus injuries associated with detection of an hematoma in the psoas are also invariably susceptible to spontaneous recovery. Iatrogenic injuries normally present spontaneous recovery when caused by traction of self-retaining retractors. Nerve injury and recovery after lateral lumbar interbody fusion with and without bone morphogenetic protein-2 augmentation: a cohort-controlled study. The indications and techniques for operative intervention of these lesions are not well described. The lumbosacral plexus also may be invaded by the malignant tumors of pelvic organs (so-called neoplastic lumbosacral plexus lesion), including rectal, prostate, cervical, and bladder cancer; involvement may be from direct, contiguous spread, or from perineural spread from the primary organ that was affected. The management of malignant lesions is controversial and beyond the scope of this review. Postoperatively the patient noticed immediate improvement in her pain, and her motor function was intact. Masses that enlarge while being observed or those presenting at a large size also should be surgically resected. There is a relative advantage to resecting asymptomatic or minimally symptomatic tumors that needs to be considered when weighing the risk/ benefit ratio of surgery. Larger tumors are more difficult to resect safely and often present with more symptoms. Many benign nerve sheath tumors tend to grow slowly, and young patients may be at some increased risk of having tumors enlarge as they age. Tumors often present at a large size in the pelvic region because they have a wide space in which to grow before becoming symptomatic. Patients with malignant lesions (either primary or secondary) tend to present differently. They often have severe pain (typically refractory to medications and narcotics) and neurologic deficits (predominantly weakness). We recommend close collaboration with experienced radiologists who can be of tremendous help in distinguishing benign from malignant nerve sheath tumors and in distinguishing tumors from other lesions that may have tumor-like appearances (including inflammatory or systematic infiltrative lesions). Patients in whom there is a suspicion of malignancy based on clinical or 138 Tumors of the Lumbosacral Plexus 883 a b c. The sheath of the tumor was opened and peeled off of the tumor with its accompanying nerve fibers. Contraindications · · Absolute: intrapelvic tumors with extensive invasion Relative: elderly age, medical comorbidities, asymptomatic small lesions that have been stable on serial imaging Disadvantages the lumbosacral plexus exposure is difficult; it requires assistance from surgical colleagues. Preoperatively, the surgeon should advise the anesthetist that the neuromuscular blockade used in induction must wear off during the early phase of the dissection so that intraoperative electrical recording can be done and the Advantages Benign nerve sheath tumors can often be resected completely and safely. Local anesthetic should be avoided due to the possibility of a nerve conduction block, which may cause errors in recording intraoperative nerve action. Occasionally, stent placement may be helpful in identifying the ureters intraoperatively in cases where the anatomy is distorted. Positioning and Exposure Tumors involving the lumbar plexus are treated slightly differently depending on anatomic considerations, such as the nerve of origin or standard bony landmarks including the anterior superior iliac spine, iliac crest, pubic symphysis, and 12th rib. For lower lumbar plexal lesions, the patient is placed in the supine position with a slight bump placed behind the lowerback/lumbar area using a rolled towel. In our practice, an access general surgeon exposes tumors involving the lumbar plexus through a retroperitoneal approach (as described in Chapter 89). A modified ilioinguinal approach is used for central or lower lumbar plexal tumors. A 2-cm width of fascia attached to the iliac crest is maintained to prevent hernia formation and to decrease pain postoperatively. Occasionally, a more posterolateral flank-type incision may be used exclusively or in conjunction with the previous incision over the iliac crest for more proximal tumors or when additional exposure is needed. For proximal exposure, the 12th rib can be resected in an extraperitoneal and extrapleural fashion. Our neurosurgical team assists with the exposure, initially to help identify and preserve cutaneous branches (including the subcostal and lateral femoral cutaneous nerves for the more proximal tumors) and later to safely identify the tumor and its parent nerve. The retroperitoneal space is entered and the peritoneal contents (and the kidney, if necessary) are retracted medially. In general, the tumors are located within 138 the psoas muscle, and blunt dissection is performed directly toward the tumor, sparing more superficially located sensory nerves (including the genitofemoral, ilioinguinal, and iliohypogastric nerves). Tumors involving the lumbosacral plexus are surgically treated with the patient in the supine position. The approach to these tumors involving the lumbosacral plexus is done by a colorectal surgeon, sometimes with the assistance of a vascular surgeon. A transabdominal transperitoneal approach is used typically through a midline incision for bigger tumors, but a Pfannenstiel incision can be used for smaller ones or in some thinner patients. Abdominal and pelvic contents are mobilized, and the presacral space is entered inbetween the bifurcation of the iliac vessels. The position of the ureters must be appreciated during the exposure and prior to tumor dissection and resection. On rare occasion, dumbbell tumors need to be treated individually via differing approaches, incorporating exposure of either the spine (laminectomies) or the sciatic notch region. Tumors of the Lumbosacral Plexus 885 Tumor Resection Once the surgical approach is done, the tumor is easily recognizable and palpable because of its size. Whenever possible, proximal and distal control of the parent nerve of the tumor is obtained to identify the normal anatomy. Other neighboring nerves or communicating branches are also identified to avoid their injury. At this time the nerve stimulator can be helpful in distinguishing among the motor and sensory nerves. Conventional nerve sheath tumors are generally resectable and should be approached with the intent of complete extirpation. The majority of lesions can be removed in toto as a single specimen separating the tumor from the nerve. The usual finding is of a tumor growing within the substance of the nerve with uninvolved fascicles splayed around the center of the mass. Schwannomas tend to be more eccentrically located and neurofibromas more centrally located. With a microsurgical technique, fascicles are gently dissected free of the tumor in the extracapsular plane. As the tumor is thus gradually exposed and the proximal and distal poles are approached, care should be taken to isolate any fascicles. Schwannomas are noted to have fascicles that run within the capsule but are unlikely to have intratumoral fascicles of significance, although they occur in the superficial layers of very large tumors. Schwannomas are thought to have a single fascicle at each pole, whereas neurofibromas may have more fascicles entering and exiting the substance of the tumor at their poles. Resection of any fascicle should not be done until the late stage of the procedure when the tumor itself is about to be definitively removed and the surgeon is confident that any fascicle cannot be maintained. Occasionally, for larger lesions, intracapsular enucleation and a piecemeal approach may be used. A longitudinal incision is made in the capsule between fascicles, and the tumor is debulked from within. We favor removing the tumor in one piece as we believe the debulking method entails a higher risk of leaving tumor behind. For plexiform lesions, debulking predominant tumor nodules may be the goal, as complete resection may not be realistic. Prostate cancer with perineural spread and dural extension causing bilateral lumbosacral plexopathy: case report. Surgery of the Lumbosacral Plexus 139 Approach to the Nerves of the Lower Extremity Jonathan D. Friedman the nerves of the lower extremity are the "neglected stepsister" of the nerves of the upper extremity. Nerve entrapment syndromes of the lower extremity are less well appreciated, and nerve injuries in the lower extremity are thought to have a poorer prognosis. Publications by Kline et al13 have demonstrated that repair of the nerves in the lower extremity can be successful. This chapter discusses the anatomy and surgical exposure of the nerves in the lower extremity, including new approaches designed to decrease approach-related morbidity. Preoperative Testing and Imaging A complete history is taken and a physical exam is performed, including a detailed neurologic workup. Patient Selection Patients present with compression neuropathies, tumors, and trauma, with injury to the nerve. Selection for surgery is based on multiple factors, including the underlying disease process, the severity of the neurologic symptoms such as severe pain or motor weakness, the focality of the pathology, and the ability of the patient to undergo surgery. The clinical aspects of nerve entrapment syndrome and the techniques of peripheral nerve repair are not discussed in this chapter. Surgical Procedure In the following subsections, each major peripheral nerve of the lower extremity is discussed, including the pertinent anatomy and the surgical approaches. Lateral Femoral Cutaneous Nerve the lateral femoral cutaneous nerve originates most frequently from the ventral rami of the second and third lumbar nerve roots. After emerging from behind the psoas muscle, the nerve lies on the iliacus muscle, passing just under the pelvic brim to exit under the inguinal ligament and over the sartorius muscle approximately one fingerbreadth medial to the anterior superior iliac spine. Approximately 5 cm beyond the iliac crest it divides into an anterior and a posterior branch, both of which pierce the fascia lata, ~ 10 cm distal to the inguinal ligament. Exposure of the lateral femoral cutaneous nerve in the pelvis is rarely indicated. When lateral femoral cutaneous nerve muscle is found in the pelvis, it is exposed by opening the abdominal wall along the anterior pelvis brim. The lateral femoral cutaneous nerve is found lying on the iliacus muscle lateral to the femoral nerve beneath the iliac fascia. The small incision and the approach through the retroperitoneal fat minimizes blood loss and approach-related morbidity. Most frequently the surgeon is interested in identifying the nerve as it passes under the inguinal ligament. Because it is often difficult to find the nerve at the level of the inguinal ligament, Indications and Contraindications Indications include injury to a nerve (partial or complete transection), tumor (benign or malignant), and entrapment syndrome. Contraindications include medical causes of neuropathy not amenable to surgical decompression, and patient health not amenable to undergoing surgery. Advantages and Disadvantages There are multiple ways to approach the peripheral nerves of the lower extremity. The larger incision approaches provide better visualization of the nerve and associated anatomy at the expense of increased approach-related morbidity from disruption of normal tissue and anatomic planes.
The head of the bed should be elevated 20 degrees bacteria definition buy simpiox 12 mg amex, creating a semi-seated position virus 68 generic simpiox 3 mg visa, to decrease bleeding into the operative field oral antibiotics for mild acne order simpiox us. Because the brachial plexus is found deep to the lateral aspect of the sternocleidomastoid vyrus 986 m2 kit discount simpiox online, the incision is planned over its lateral boarder antibiotics how long order generic simpiox, which is easily palpable. Depending on the details of the case, it is often prudent to prepare for a combined supraclavicular and infraclavicular approach. After sharply incising the superficial investing fascia layer, supraclavicular fat is dissected and pulled away laterally from the posterior edge of the sternocleidomastoid muscle. The branches of the supraclavicular cervical plexus and external jugular vein are identified and dissected laterally. The external jugular vein and larger vessels can almost always be mobilized safely unless they are encased in tumor or prior exposure to radiation complicates the situation. During dissection along the upper part of the posterior cervical triangle, great caution must be taken to avoid injury to the spinal accessory nerve where the nerve emerges from just above the midpoint of the posterior border of the sternocleidomastoid muscle. The posterior belly of the omohyoid muscle is divided and pulled laterally after it is tagged with sutures for later reapproximation. As the posterior cervical triangle fat is dissected from the edges of the sternocleidomastoid muscle and clavicle, the transverse cervical artery and vein, which cross the plexus, can be seen, ligated, and divided. When the sternocleidomastoid muscle is retracted medially, the phrenic nerve can be identified as it runs along the superolateral border on the ventral surface of the anterior scalene muscle. The phrenic nerve is an important landmark for locating the C5 spinal nerve, which unites with C6 to form the upper trunk of the brachial plexus. The nerve stimulator, set at 1 mA, can be used to stimulate the phrenic nerve, causing contraction of the ipsilateral hemidiaphragm. The phrenic nerve is dissected and mobilized medially with a vascular loop around the nerve so that the upper trunk can be dissected. It emerges from the posterior border of the sternocleidomastoid muscle, loops around it, and can be traced proximally to identify C4 inferiorly to the C5 spinal nerve. Proximal dissection of the C5 nerve requires the resection of the transverse process with a high-speed drill or a No. Venous plexus around the spinal nerve close to the foramen requires meticulous hemostasis with bipolar, Gelfoam with thrombon, or Surgicel. Special attention is required during dissection of C5 at the foramen to avoid injuring the dorsal scapular nerve, which originates from the posterior aspect of C5, lateral to the small branch given off, forming the long thoracic nerve. The long thoracic nerve arises from the dorsal surface of the C6 spinal nerve with contributions from C5 and C7. It pierces through the middle scalene muscle and runs posterior to the brachial plexus and continues inferiorly to innervate the serratus anterior muscle in the chest wall. The nerve to the subclavius muscle arises from the anterior aspect of the upper trunk. This nerve has no clinical significance except that it is the origin of the phrenic nerve. During dissection along the posterolateral aspect of the upper trunk, the suprascapular nerve can be identified and isolated from the upper trunk. It runs toward the scapular notch, level with the clavicle and the suprascapular artery and vein. The C7 spinal nerve emerges from between the anterior and middle scalene muscles inferior to the C5 and C6 spinal nerves. To improve the exposure of the proximal middle trunk and C7 spinal nerve, the anterior scalene muscle can be resected while protecting the phrenic nerve. The lateral portion of clavicular insertion of the sternocleidomastoid muscle is detached from the clavicle, and retraction of the subclavian artery inferiorly by using a vein retractor can further expose C8, T1, and the lower trunk. A planned incision over the lateral aspect of the sternocleidomastoid muscle provides access to the supraclavicular plexus. The surgeon should be able to manipulate the position of the arm to improve surgical exposure. Meticulous hemostasis can be achieved through the use of bipolar cautery throughout the dissection. The placement of tourniquets around the extremities is seldom required, and their use can cause ischemia to tissue or further compressive and ischemic damage to an already injured nerve. Our generally preferred method of nerve grafting is to use the sural nerve due to its length and minimal morbidity from harvesting. In cases where it is known or highly anticipated that a graft will be needed, we prefer to harvest the graft with the patient in the prone position prior to starting the brachial plexus operation. Preoperative physical examination and electrodiagnostic studies are critically important for predicting the intraoperative electrical recordings and thus the need for a graft. In cases where it is difficult to predict the need for nerve grafting, we prefer to make this decision intraoperatively at the time of brachial plexus exploration. The sural nerve graft harvest can then be performed in another step with subsequent interfascicular graft repair. The incision curves parallel to the clavicle toward the proximal part of the deltopectoral groove. A pure supraclavicular approach does not require an incision past the lateral third of the clavicle. That being said, the marked line should also extend below the clavicle, toward the axillary crease, if it becomes necessary to expose the infraclavicular portion of the brachial plexus. Dissection After the skin incision is made, a thin layer of platysma muscle is encountered and sharply incised. The posterior cervical triangle 130 Supraclavicular Approach to Brachial Plexus Surgery. After the sternocleidomastoid muscle is retracted medially, the phrenic nerve is found overlying the superficial surface of the scalenus medius. The phrenic nerve can be traced proximally to define C4 and C5 spinal nerves from C6. Resection of the anterior scalene muscle facilitates the mobilization of the subclavian artery. Special caution must be taken when dissecting around the T1 spinal nerve to prevent injury to the vertebral artery, cervicothoracic ganglion (stellate ganglion), apex of pleura, and thoracic duct in left-side dissection. If the surgeon inadvertently enters the pleura during dissection of the T1 spinal nerve, the pleura can be repaired with 4-0 silk sutures and controlled ventilation by the anesthesiologist. Plan to obtain an intraoperative chest X-ray in the operating room after closure for chest tube placement if there is significant pneumothorax. There are no nerve branches originating from the middle or lower trunks in the supraclavicular region. The clavicle is dissected circumferentially by isolating both the subclavius muscle and the vessel beneath the clavicle. A moistened sponge gauge is placed around the clavicle and clamped with a large hemostat, which can be used to pull the clavicle inferiorly, giving a better view of the structures underneath the clavicle. Anterior and posterior divisions from three trunks are located under the clavicle. Donor Nerve Graft Harvesting the most common sources of donor nerve grafts are the sural nerves from both lower extremities. A longitudinal incision is made at ankle level between the Achilles tendon and medial malleolus toward the popliteal fossa, and then along the posterior calf where it lies subcutaneously. The entire length of the sural nerve can be harvested as it generally forms from the peroneal. Most injuries are lesions in continuity, along with severe internal disruption and formation of the neuroma mass. The dissection should be extended proximally and distally to the injured nerve segment, as well as to other neural elements of the brachial plexus, so as to understand the extent of the injury and its relationship to the surrounding anatomy. It is essential that proper decisions are made as to which proximal lead-out grafts go with what distal segments. Determining the number of nerve grafts to be used and their proper lengths will minimize tension at the repair sites. These are important factors to address, as they have a significant impact on functional recovery. This is done by extending the dissection of the nerve longitudinally along the nerve, mobilizing the joint, and performing nerve transposition, which provides a more direct route to the nerve. Most stretch injuries of the supraclavicular brachial plexus cannot be repaired by direct suture repair. If avulsed spinal nerves are identified, proximal dissection at the level of the foramen is necessary so that the surgeon may find a potential lead-out stump for nerve graft repair. If complete spinal root avulsion is encountered, it may not be possible to identify proximal lead-outs for direct nerve grafting, in which case the surgeon must perform neurotization using the descending cervical plexus, distal spinal accessory nerve, or intercostal nerves to the musculocutaneous nerve. Surgeons must be prepared to extend their exploration into the infraclavicular brachial plexus to obtain adequate access when necessary. Proper preoperative planning including physical examination, electrodiagnostic studies, and magnetic resonance imaging are critical in obtaining good long-term neurologic outcomes. Surgical Repair Laceration Transection or acute laceration injuries to the plexus are best repaired immediately while inflammation and nerve regeneration has not yet begun. Acute exploration and direct end-to-end suture repair (neurorrhaphy) of supraclavicular brachial plexus injuries that are the result of sharp laceration have very favorable functional surgical outcomes. If bluntly transected injuries from motor blades or chain saws are observed during acute exploration for vascular repair, each stump needs to be tacked down to the adjacent soft tissue for future repair. This will maintain the length of the lesion and minimize the length of any nerve grafts that are required after resection of both ends of the nerve stumps. Posttraumatic neuromas must be resected until healthy fascicles can be observed in subsequent surgeries. Kim Infraclavicular brachial plexus injury is caused by stretch injuries, contusive injuries to the cords, cords and nerve lesions with associated axillary artery injury, shoulder dislocation or fracture, and humeral fracture. Infraclavicular stretch injuries often spare shoulder function, but damage extends from divisions of the cords to more distal nerves. With the infraclavicular approach, the surgeon has complete access to the anterior and posterior divisions; the lateral, posterior, and medial cords of the brachial plexus and their branches; and the musculocutaneous, subscapular, thoracodorsal, axillary, radial, ulnar, median, lateral, and medial pectoral nerves. The divisions of all three trunks help form the three cords of the brachial plexus. The anterior divisions of the upper and middle trunks unite to form the lateral cord, distal to the clavicle. The anterior division of the lower trunk continues to form the medial cord, which is medial to the axillary artery. All posterior divisions of the three trunks unite to form the posterior cord of the brachial plexus, which is situated behind the axillary artery. The musculocutaneous nerve descends into the biceps and the brachialis after supplying branches to the coracobrachialis muscle. The lateral pectoral nerve arises from the lateral cord and sends a ramus to the medial pectoral nerve, which forms a loop and penetrates through the clavipectoral fascia to innervate the pectoralis major muscle. The upper subscapular nerve is a small branch that runs posterior to the axillary artery and innervates the upper part of the subscapular muscle. The distal division, cords (yellow) and terminal branches are accessible via the infraclavicular approach. The lower subscapular nerve innervates the lower part of the subscapularis and teres major muscles. The axillary nerve generally arises from the posterior cord but can also arise from the posterior divisions of the upper and middle trunks. It runs anterior to the subscapularis muscle and passes through the quadrilateral space, which is bounded above by the subscapularis and teres minor muscles, below by the teres major muscle, medially by the long head of the triceps, and laterally by the surgical neck of the humerus. The axillary nerve innervates the articular shoulder joint, the deltoid and teres minor muscles, and the skin overlying the deltoid. The radial nerve is a large terminal branch of the posterior cord, which runs inferiorly toward the humeral groove and wraps around the humerus. Meticulous hemostasis can be achieved through the use of the bipolar cautery throughout the dissection. Placement of tourniquets around the extremities is seldom required, and their use can cause ischemia to tissue or further compressive and ischemic damage to an already injured nerve. The cephalic vein is typically ligated as it crosses the axillary vein close to the clavicle. Dissection After the subclavicular muscle and vein are dissected and ligated, the clavicle can be mobilized and retracted superiorly by using a moistened sponge, which is placed under and around the clavicle to expose the infraclavicular portion of the brachial plexus. After self-retaining retractors, such as an Adson, are placed between the deltoid and pectoralis major muscles along the deltopectoral groove, the clavipectoral fascia is identified and then divided to expose the origin of the pectoralis minor muscle at the coracoid process. The tendon belonging to the pectoralis minor muscle is divided after being tagged with two sutures on either side for later approximation. Distal exposure is gained by elevating and pulling the pectoralis major muscle inferiorly on a sling with a sponge gauge to expose a broad expanse of the infraclavicular space. The infraclavicular incision starts at the superior margin of the deltopectoral groove and extends distally to the axillary crease. The supraclavicular portion should always be planned as it courses over the lateral aspect of the sternocleidomastoid muscle down to its attachment at the clavicle. Division of the pectoralis minor muscle tendon at the coracoid process enables complete dissection of the infraclavicular brachial plexus. The lateral cord gives off the lateral pectoral nerve and branches into the musculocutaneous nerve and lateral cord and contributes to the median nerve. The musculocutaneous nerve, a terminal branch of the lateral cord, dives into the biceps and brachialis after piercing and supplying the coracobrachialis muscle. The posterior cord is formed by the posterior divisions of all three trunks and lies posterior to the axillary artery. Several subscapular branches arise, usually from the posterior cord or axillary, and run inferiorly and obliquely, innervating the subscapularis and teres major muscles. The thoracodorsal nerve arises from the posterior cord, innervating the latissimus dorsi.
Purchase simpiox with american express. Viral evolution frog-killing fungi and antibiotic resistance reports - Microbial Minutes 04/09/18.
References
- Garcia-Donaire J, Alcazar J: Ischemic nephropathy: detection and therapeutic intervention, Kidney Int 68(Suppl 99):S131nS136, 2005.
- Kelly WK. Epothilones in prostate cancer. Urol Oncol 2011;29(4):358-365.
- Linggood RM, Hsu DW, Efird JT, Pardo FS. TGF alpha expression in meningioma -tumor progression and therapeutic response. J Neurooncol 1995; 26:45-51.
- Santoro N, Torrens J, Crawford S, et al: Correlates of circulating androgens in mid-life women: the study of womenis health across the nation, J Clin Endocrinol Metab 90(8):4836n4845, 2005.
- Farwell D, Patel NR, Hall A, Ralph S, Sulke AN. How many people with heart failure are appropriate for biventricular resynchronization? Eur Heart J 2000;21(15):1246-1250.
- Zhang JH, Sampogna S, Morales FR, Chase MH. Age-related changes of hypocretin in basal forebrain of guinea pig. Peptides 2005;26(12):2590-6.