Charles M. Little, DO, FACEP
- Program Coordinator, Pandemic Taskforce
- University of Colorado Hospital
- Associate Professor
- Division of Emergency Medicine
- University of Colorado Denver School of Medicine
- Aurora, Colorado
This inflammatory dermatosis results in chronic eruption of shiny purple papules with white striae on the vulva heart attack numbness buy nifedipine in united states online. Similar lesions are often found on the flexor surfaces blood pressure pills make you tired order nifedipine 20 mg mastercard, and mucous membrane of the oral cavity mutemath blood pressure order cheapest nifedipine and nifedipine. It generally occurs in women in their 50s or 60s arrhythmia research summit order nifedipine 30 mg overnight delivery, and it is associated with a 3% to 5% risk of vulvar skin cancer arrhythmia consultants of connecticut nifedipine 20 mg order visa. Vulvar psoriasis may be a feature of psoriasis-a very common skin rash that affects up to 2% of the population. There are several different types, but the usual form appears as silvery-red scaly patches over the elbows and knees. Vulvar psoriasis can occur as part of more general disease but in some people, it affects only the vulva. This disorder may begin with something that simply rubs, irritates, or scratches the skin, such as clothing. Or, intense pruritis may develop secondary to atopic dermatitis, psoriasis, neuropathic pain, or psychologic disorders. The constant scratching causes an inflammatory reaction with subsequent skin thickening. The appearance depends on whether the patient rubs the area (lichenfication) or scratches the area (excoriations). They may also report dysuria, dyspareunia, and vulvar pain, and feel that the skin of their vulva is tender, bumpy, irritated, or thickened. Physical Examination these disorders range in appearance from erythematous plaques to hyperkeratotic white plaques to erosions and ulcers (Table 13-1). Occasionally, petechiae and/or ecchymoses are present as a result of trauma from scratching. Colpoposcopy and directed biopsy can also be used to evaluate and identify vulvar and vaginal lesions. Ulcererations may be seen with aphthous ulcers, Behçet syndrome, Crohns disease, erythema multiforme, bullous pemphigoid, and plasma cell vulvitis. Vulvovaginal irritation and pruritis may be seen in yeast, folliculitis, trichomoniasis, contact dermatitis, and drug reactions. The differential diagnosis also includes premalignant and malignant disease such as vulvar and vaginal intraepithelial neoplasia, squamous cell carcinoma, and Paget disease of the vulva. Patients should avoid tight-fitting clothes; pantyhose; panty liners; scented soaps and detergents; bubble baths; washcloths; and feminine sprays, douches, and powders. They should use mild, unscented detergents and soaps such as Dove or Cetaphil, and take morning and evening tub baths without additives. In general, there is no role for topical estrogens or testosterone in the treatment of these disorders; however, low-dose vaginal estrogen is an effective treatment for concomitant genital urinary syndrome of menopause. Similarly, surgical management is generally not indicated in treatment of these disorders. Cysts can originate from occlusion of pilosebaceous ducts, sebaceous ducts, and apocrine sweat glands. Treatment of benign cystic and solid tumors is needed only if the lesions become symptomatic or infected. These cysts usually result from occlusion of a pilosebaceous duct or a blocked hair follicle. They are lined with squamous epithelium and contain tissue that would normally be exfoliated. These solitary lesions are normally small and asymptomatic; however, if these become superinfected and developed into abscesses, incision and drainage or complete excision is the treatment. As with any cyst, these can become superinfected with local flora and require treatment with incision and drainage. Fox-Fordyce disease is an infrequently occurring chronic pruritic papular eruption that localizes to areas, where apocrine glands are found. Hidradenitis suppurativa is a skin disease that most commonly affects areas bearing apocrine sweat glands or sebaceous glands, such as the underarms, breasts, inner thighs, groin, and buttocks. Initial treatment for hidradenitis includes antimicrobial skin washes and antibiotic ointments. As in the axillary region, if these cysts become infected and form multiple abscesses, excision or incision and drainage are the treatments of choice. When conservative measures fail, persistent or recurrent paraurethral cysts can be treated with simple marsupialization or excision. They are mucus-secreting glands with ducts that open just external to the hymenal ring. If the cyst remains small (1 to 2 cm) and is asymptomatic, it can be left untreated and will often resolve on its own or with sitz baths. These abscesses are the result of polymicrobial infections, but they are also occasionally associated with sexually transmitted infections. These abscesses can become quite large, causing exquisite pain and tenderness and associated cellulitis. However, simple incision and drainage can often lead to recurrence; therefore, one of the two methods can be used. Word catheter placement is commonly performed in the emergent setting or in the office. This method involves making a small incision (5 mm) to drain and irrigate the cyst or abscess. The balloon is left in place for 4 to 6 weeks, being serially reduced in size, while epithelialization of the cyst and tract occurs. A small-gauge needle is inserted into the opposite end and 2 to 4 mL of water is injected. The inflated balloon remains inside the cyst for 4 to 6 week until an epithelialized tract is formed to prevent blockage of the duct to recur. With either treatment, warm sitz baths several times per day are recommended both for pain relief and to decrease healing time. Adjunct antibiotic therapy is only recommended when the drainage is positive for Neisseria gonorrhoeae, which occurs approximately 10% of the time. Concomitant cellulitis or an abscess that seems refractory to simple surgical treatment should also be treated with antibiotics that cover skin flora, primarily Staphylococcus aureus. They are found most commonly in the anterior lateral aspects of the upper part of the vagina. However, patients may present in adolescence with dyspareunia or difficulty inserting a tampon. When the removal is necessary, an intravenous pyelogram and cystoscopy should be performed preoperatively to locate the position of the bladder and ureters relative to the cyst. Urethral diverticula, ectopic ureters, and vaginal and cervical cancer should be ruled out. Because of the potential for significant bleeding during excision, vasopressin may be used to maintain hemostasis during the procedure. Lipomas are soft pedunculated or sessile tumors composed of mature fat cells and fibrous strands. Cherry hemangiomas are elevated soft red papules, also known as Campbell De Morgan spots or senile angiomas; they contain an abnormal proliferation of blood vessels. Urethral caruncles and urethral prolapse present as small, red, fleshy tumors found at the distal urethral meatus. These occur almost exclusively in postmenopausal women as a result of genital urinary syndrome of menopause. In case of a uterine didelphys with a double vagina, a double cervix (bicollis) may be found, but this does not arise in isolation. These are caused by intermittent blockage of an endocervical gland and usually expand to no more than 1 cm in diameter. Nabothian cysts are more commonly found in menstruating women and are usually asymptomatic. Most often, nabothian cysts are discovered on routine gynecologic examination and require no treatment. These cysts differ from nabothian cysts in that they tend to lie deeper in the cervical stroma and on the external surface of the cervix. These cysts tend to be red or purple in color, and the patient will often have associated symptoms of endometriosis such as cyclic pelvic pain and dyspareunia. When symptomatic, cervical polyps usually cause intermenstrual or postcoital spotting rather than pain. Although cervical polyps are not usually considered a premalignant condition, they are generally removed to decrease the likelihood of masking irregular bleeding from another source such as cervical cancer, fibroids, adenomyosis, endometrial polyps, endometrialintraepithelial neoplasia, and endometrial cancer. The removal of pedunculated cervical polyps is typically quick and easily performed in the office. However, sessile (broad based) polyps or larger polyps may require removal with electrocautery in the office or the operating room. Hysteroscopy may also be helpful in distinguishing cervical polyps from endometrial polyps. Cervical leiomyomas can cause symptoms of intermenstrual bleeding similar to both uterine fibroids and cervical polyps. Depending on their location and size, these can also cause dyspareunia and bladder or rectal pressure. Fibroids of the cervix can cause problems in pregnancy and may lead to hemorrhage, poor dilation of the cervix, malpresentation, or obstruction of the birth canal. When evaluating an asymptomatic cervical fibroid, the possibility of cervical cancer should be ruled out, and then the fibroid can be followed with routine gynecologic care. Symptomatic fibroids can be surgically removed but, depending on their location and size, hysterectomy rather than myomectomy may be required. Less frequently, cervical stenosis can result from obstruction with a neoplasm, polyp, or fibroid. Cervical stenosis is typically asymptomatic and does not affect menstruation or fertility. However, if egress from the uterus is completely or partially blocked, oligomenorrhea, amenorrhea, dysmenorrhea, or an enlarged uterus may result. Cervical stenosis can also impede access to the endocervical and endometrial canals for diagnostic and therapeutic procedures. When symptoms are present or access to the endocervical or endometrial canals are needed, cervical stenosis can be treated by gentle dilation of the cervix or by performing a cruciate incision over the external os. Prolonged patency can be improved by leaving a catheter in the cervical canal for a few days after the stenosis is relieved. Patients are genetically female with normal ovarian function and normal secondary sexual characteristics. There is a limited role for vaginal estrogens and surgery in the treatment of these disorders. When symptomatic, the stenosis can be treated with gentle dilation of the cervical canal. She has had two lifetime sexual partners and has been with her last partner for 5 years. She has always had normal periods and Pap smears, and has never had a sexually transmitted infection. Expectant management Word catheterization I&D (incision and drainage) Marsupialization Excision 3. She is having difficulty sitting at work, and has not been able to exercise for 3 days due to pain. If this patient had been 46 years old at the first onset of her cyst, what would be required Review of her outside medical records reveals five episodes of vulvar pruritus that were treated with oral and vaginal antifungal medication. The patient says these helped minimally, but her intense pruritus has been persistent for more than a year. She was married for 35 years, but is now widowed and has not been sexually active in 3 years. You examine her and find a thin white atrophic epithelium and a contracted, small introitus. An area of hypopigmentation surrounds the labia and the anus in a figure-of-eight pattern. Collect fungal cultures Screen for gonorrhea and chlamydia Prescribe a longer course of oral fluconazole (Diflucan) Check a fasting glucose level Perform a vulvar biopsy 2. However, when attempting the pelvic examination, you are unable to locate a vaginal introitus. On physical examination, she has age-appropriate breast and pubic hair development and normal external genitalia. You obtain a transabdominal ultrasound, which reveals a hematocolpos and hematometra. It typically appears as a midline protrusion of the anterior vaginal wall into the vagina and, if severe, through the introitus. Cystoceles and other pelvic organ prolapse occur most commonly in older women and in women who have had multiple vaginal deliveries. However, these are the most common cause of cutaneous cysts and are typically small and solitary. Answer A: In this case, where the cyst is largely asymptomatic, and there is no sign of abscess or superinfection, expectant management is appropriate. Leaving the Word catheter in place for several weeks gives the new tract time to reepithelialize hopefully resulting in a means of long-term drainage. Marsupialization is typically reserved for patients in whom the Word catheter has failed. Answer E: Although yeast infections are a common cause of vaginitis in women, this patient has been adequately treated for yeast vaginitis, but still has persistent symptoms. Her wet prep does also not support the diagnosis of yeast infection because minimal pseudohyphae are found.
There is a slight decrease in the concentration of platelets prehypertension levels generic nifedipine 20 mg on-line, probably secondary to increased plasma volume and an increase in peripheral destruction blood pressure xanax withdrawal purchase generic nifedipine line. Although in 7% to 8% of patients arrhythmia education inc nifedipine 30 mg buy otc, the platelet count may be between 100 and 150 million/mL blood pressure medication photosensitivity order nifedipine us, a drop in the platelet count below 100 million/mL over a short time is not normal and should be investigated promptly 2013 nifedipine 30 mg. Pregnancy is considered to be a hypercoagulable state with an increase in the number of thromboembolic events. The increased rate of thromboembolic events in pregnancy may also be secondary to the other elements of Virchow triad, that is, an increase in venous stasis and vessel endothelial damage. The increased estrogen is produced primarily by the placenta, with the ovaries contributing to a lesser degree. Unlike estrogen production in the ovaries, where estrogen precursors are produced in ovarian theca cells and transferred to the ovarian granulosa cells, estrogen in the placenta is derived from circulating plasma-borne precursors produced by the maternal adrenal glands. Fetal well-being has been correlated with maternal serum estrogen levels, with low estrogen levels being associated with conditions such as fetal death and anencephaly. Eventually, the placenta takes over progesterone production, and the corpus luteum degrades into the corpus albicans. Progesterone causes relaxation of smooth muscle, which has multiple effects on the gastrointestinal, cardiovascular, and genitourinary systems. First, estrogen stimulates thyroid binding globulin, leading to an elevation in total T3 and T4, but free T3 and T4 remain relatively constant. Musculoskeletal and Dermatologic the obvious change in the center of gravity during pregnancy can lead to a shift in posture and lower back strain, which worsens throughout pregnancy, particularly during the third trimester. Numerous changes occur in the skin, including spider angiomata and palmar erythema secondary to increased estrogen levels, and hyperpigmentation of the nipples, umbilicus, abdominal midline (the linea nigra), perineum, and face (melasma or chloasma) secondary to increased levels of the melanocyte-stimulating hormones and the steroid hormones. Pregnancy is also associated with carpal tunnel syndrome, which results from compression of the median nerve. The caloric requirement is increased by 300 kcal/day during pregnancy and by 500 kcal/day when breastfeeding. Thus, pregnancy is not the caloric equivalent of eating for two; more accurately, it is approximately eating for 1. Overweight women are advised to gain less, between 15 and 25 lb; underweight women are advised to gain more, 28 to 40 lb. Unfortunately, a large proportion of women gain more than the recommended amount, which contributes to a number of complications in pregnancy plus postpartum weight retention and downstream obesity. It is the responsibility of each prenatal care provider to review diet and exercise during pregnancy. In addition to the increased caloric requirements, there are increased nutritional requirements for protein, iron, folate, calcium, and other vitamins and minerals. Many patients develop iron deficiency anemia because of the increased demand on hematopoiesis both by the mother and by the fetus. These are designed to compensate for the increased nutritional demands of pregnancy. Furthermore, any patient whose hematocrit falls during pregnancy is advised to increase iron intake with oral supplementation (Table 1-2). They include a series of outpatient office visits that involve routine physical examinations and various screening tests that occur at different points in the prenatal care. Important issues of prenatal care include initial patient evaluation, routine patient evaluation, safety and housing, nutrition and food security, disease states during the pregnancy, and preparing for the delivery. It should occur early in the first trimester, between 6 and 10 weeks, although occasionally patients will not present for their initial prenatal visit until later in their pregnancy. After this, an obstetric history of prior pregnancies, including date, outcome. Finally, a complete medical, surgical, family, and social history should be obtained. The pelvic examination includes a Pap smear according to standard cervical cancer screening guidelines and cultures for gonorrhea and chlamydia. Accurate dating is crucial for all subsequent obstetric evaluations and interventions. A urine pregnancy test should be sent if the patient is not entirely certain she is pregnant. Although there is some debate over the use of routine toxoplasma titers, they are often ordered as well. In addition to this battery of tests, there are a variety of other screens offered to high-risk patients (Table 1-4). Initial Screens in Specific High-Risk Groups High-Risk Group African American, Southeast Asian Family history of genetic disorder. Maternal blood pressure decreases during the first and second trimesters and slowly returns to baseline during the third trimester; elevation may be a sign of preeclampsia. Maternal weight is followed serially throughout the pregnancy as a proxy for adequate nutrition. Also, large weight gains toward the end of pregnancy can be a sign of fluid retention and preeclampsia. Measurement of the uterine fundal height in centimeters corresponds roughly to the weeks of gestation. At each visit, the patient is asked about symptoms that indicate complications of pregnancy. These symptoms include vaginal bleeding, vaginal discharge or leaking of fluid, and urinary symptoms. In addition, after 20 weeks, patients are asked about contractions and fetal movement. Vaginal bleeding is a sign of possible miscarriage or ectopic pregnancy in the first trimester and of placental abruption or previa as the pregnancy advances. Vaginal discharge may be a sign of infection or cervical change, whereas leaking fluid can indicate ruptured fetal membranes. While irregular (Braxton Hicks) contractions are common throughout the third trimester, regular contractions occurring more frequently than five or six per hour may be a sign of preterm labor and should be assessed. First-Trimester Visits During the first trimester, patients-particularly nulliparous women-need to be familiarized with pregnancy. The symptoms of pregnancy and what will occur at each prenatal visit should be reviewed. At the second prenatal visit, all of the initial laboratory test results should be reviewed with the patient. Those with poor weight gain or decreased caloric intake secondary to nausea and vomiting may be referred to a nutritionist. Patients treated for infections noted at the initial prenatal visit should be cultured for test of cure. Second-Trimester Visits During the second trimester, much of the screening for genetic and congenital abnormalities is done. This allows a patient to obtain an elective termination if there are abnormalities. The addition of inhibin A to this screening test further enhances the ability to detect abnormalities and is known as the quad screen. Historically, these maternal analytes combined with ultrasound were the only options for genetic screening. However, an alternative is now available and is being offered to patients with increasing frequency. Most patients have resolution of their nausea and vomiting by the second trimester, although some continue with these symptoms throughout their pregnancy. Patients will begin to have occasional Braxton Hicks contractions and, if these contractions become regular, the cervix is examined to rule out preterm labor. Prenatal visits increase to every 2 to 3 weeks from 28 to 36 weeks and then to every week after 36 weeks. Either as a routine or if there is any question, an office ultrasound may be used at 35 to 36 weeks to confirm fetal presentation. In the setting of breech presentation, women are offered external cephalic version of the fetus at 37 to 38 weeks of gestation. Beyond 37 weeks, which is considered term, the cervix is usually examined at each visit. Because a vigorous examination of the cervix, known as "sweeping" or "stripping" the membranes, has been demonstrated to decrease the probability of progressing postterm or requiring an induction of labor, this is commonly offered at all term pregnancy prenatal visits. Third-Trimester Laboratory Test Results At 27 to 29 weeks, the third-trimester laboratory test results are ordered. Patients with a hematocrit below 32% to 33% (hemoglobin <11 mg/dL) are usually started on iron supplementation. Because this will cause further constipation, stool softeners are given in conjunction. It consists of giving a 50-g oral glucose loading dose and checking serum glucose 1 hour later. It consists of a fasting serum glucose measurement and then administration of a 100-g oral glucose loading dose. The serum glucose is then measured at 1, 2, and 3 hours after the oral dose is given. This test is indicative of gestational diabetes if there is an elevation in two or more of the following threshold values: the fasting glucose, 95 mg/dL; 1 hour, 180 mg/dL; 2 hour, 155 mg/dL; or 3 hour, 140 mg/dL. In high-risk populations, vaginal cultures for gonorrhea and chlamydia are repeated late in the third trimester. Patients who have a positive culture should be treated with intravenous penicillin when they present in labor to prevent potential neonatal group B streptococcal infection. Mild exercise-particularly stretching- may release endorphins and reduce the amount of back pain. For patients with severe back pain, muscle relaxants or, occasionally, narcotics can be used. Laxatives can be used, but are usually avoided in the third trimester because of the theoretical risk of preterm labor. Dehydration may cause increased contractions, and patients should be advised to drink many (10 to 14) glasses of water per day. Regular contractions, as often as every 10 minutes, should be considered a sign of preterm labor and should be assessed by cervical examination. If a patient has had several days of contractions and no documented cervical change, this is reassuring to both the obstetrician and the patient that delivery is not imminent. As mentioned above, dehydration may lead to uterine contractions, possibly secondary to cross-reaction of vasopressin with oxytocin receptors. Severe edema of the face and hands may be indicative of preeclampsia and merits further evaluation. Patients with reflux should be started on antacids, advised to eat multiple small meals per day, and should avoid lying down within an hour of eating. For patients with continued symptoms, H2 blockers or proton pump inhibitors can be given. Congestion of the pelvic vessels combined with increased abdominal pressure with bowel movements secondary to constipation can lead to hemorrhoids. Hemorrhoids are treated symptomatically with topical anesthetics and steroids for pain and swelling. Prevention of constipation with increased fluids, increased fiber in the diet, and stool softeners may prevent or decrease the exacerbation of hemorrhoids. As long as these substances are nontoxic, the patient is advised to maintain adequate nutrition and encouraged to stop ingesting the inedible items. However, if the patient has been consuming toxic substances, immediate cessation along with a toxicology consult is advised. This pain is likely secondary to the rapid expansion of the uterus and stretching of the ligamentous attachments, such as the round ligaments. This is often selflimited but may be relieved with warm compresses or acetaminophen. However, the most likely cause of urinary frequency during pregnancy is increasing compression of the bladder by the growing uterus. If no infection is present, patients can be assured that the increased voiding is normal. The relaxation of the venous smooth muscle and increased intravascular pressure, probably both, contribute to the pathogenesis. Elevation of the lower extremities or the use of pressure stockings may help reduce existing varicosities and prevent more from developing. If the problem does not resolve by 6 months postpartum, patients may be referred for surgical therapy. Parents can be screened for common diseases such as cystic fibrosis, TaySachs disease, sickle cell disease, and thalassemia. If both parents are carriers of recessive genetic diseases, the fetus can then be diagnosed. The fetus can be imaged and many of the congenital anomalies diagnosed via second-trimester ultrasound. First- and second-trimester genetic screening and prenatal diagnosis is discussed further in Chapter 3. Other fetal testing includes fetal blood sampling, fetal lung maturity testing, and assessment of fetal wellbeing. To detect fetal malformations, most patients undergo a routine screening ultrasound at 18 to 20 weeks. Of note, most patients will think of this ultrasound as the time to find out the fetal sex. It is useful to clarify this point with patients to establish proper expectations for the ultrasound. In high-risk patients, careful attention is paid to commonly associated anomalies such as cardiac anomalies in pregestational diabetics.
While several approaches have been identified in experimental models to reduce reperfusion injury blood pressure 80 over 50 purchase nifedipine line, none have exhibited sufficient benefit to warrant regular clinical use blood pressure medication lower testosterone generic 20 mg nifedipine mastercard. In addition heart attack urine purchase 20 mg nifedipine, much of the data for these therapeutics in human studies is inconclusive regarding the long-term effects of treatment heart attack 60 generic nifedipine 20 mg buy on-line. However blood pressure j curve generic 30 mg nifedipine free shipping, given the therapeutic benefit of reducing reperfusioninduced cardiac damage evidenced by significant reductions in infarct size by mechanical and pharmacological therapies, optimal use of these therapies is feasible. Furthermore, the promising results from pharmacologic agents targeted at optimizing energy metabolism in the heart following ischemic damage will undoubtedly play a role in future therapeutic interventions. Historical perspective on the pathology of myocardial ischemia/reperfusion injury. Contribution of Na+/H+ exchange to Na+ overload in the ischemic hypertrophied hyperthyroid rat heart. Targeting fatty acid and carbohydrate oxidation a novel therapeutic intervention in the ischemic and failing heart. Regulation of signal transduction by reactive oxygen species in the cardiovascular system. The mitochondrial permeability transition pore: molecular nature and role as a target in cardioprotection. Time course of endothelial dysfunction and myocardial injury during myocardial ischemia and reperfusion in the cat. Myocardial ischemia/reperfusion-injury: a clinical view on a complex pathophysiological process. Nrf2 as a master redox switch in turning on the cellular signaling involved in the induction of cytoprotective genes by some chemopreventive phytochemicals. Preconditioning with ischemia: a delay of lethal cell injury in ischemic myocardium. Postconditioning: a simple, clinically applicable procedure to improve revascularization in acute myocardial infarction. Ischemic postconditioning during primary percutaneous coronary intervention: the effects of postconditioning on myocardial reperfusion in patients with st-segment elevation myocardial infarction (post) randomized trial. The study design for a multicenter randomized double-blinded controlled clinical trial the ripheart-study. Targeting an antioxidant to mitochondria decreases cardiac ischemia-reperfusion injury. Erythropoietin protects the myocardium against reperfusion injury in vitro and in vivo. Myocardial metabolic and hemodynamic effects of dichloroacetate in coronary artery disease. Targeting fatty acid and carbohydrate oxidation - a novel therapeutic intervention in the ischemic and failing heart. Systematic review of the efficacy and safety of perhexiline in the treatment of ischemic heart disease. This condition is mainly caused by diastolic dysfunction that may even be present in compensated hypertrophy. In general, metabolic remodeling in cardiac hypertrophy and failure is characterized by a shift away from energy production to activation of biosynthetic pathways required for structural remodeling processes such as ventricular hypertrophy and fibrosis. Particularly, fatty acid oxidation is decreased and may not be sufficiently compensated for given the lack of increase in glucose oxidation. These results are also consistent with findings in spontaneously hypertensive rats [18,12], and in rats with abdominal constriction [10,9], but not with those in Dahl salt-sensitive rats [11] and in rats with myocardial infarction [14]. It is unlikely that these differences can be explained by methodological differences. This substrate selection pattern resembles that of the fetal heart and is often considered part of the reactivation of the fetal gene program. Therefore, the phenomenon of substrate switch has been suggested as an adaptive response that shifts cardiac energy metabolism to a more favorable phenotype [22,23]. Many attempts have been made to evaluate the role of the cardiac substrate switch. This interaction is also referred to as the Randle cycle and has been exploited to modulate cardiac substrate selection [24]. In the presence of systolic dysfunction, cardiac glucose uptake was found to be decreased following aortic constriction in mice [7] but unchanged in rats with myocardial infarction [15], and increased in Dahl salt-sensitive rats [11]. In compensated hypertrophy, induced by abdominal aortic constriction, glycolysis was modestly increased without changes in glucose oxidation [9,8]. By assessing substrate oxidation at various time points following aortic constriction in rats, we observed that cardiac glucose oxidation tended to increase initially, but was unchanged in the stage of compensated hypertrophy and ultimately decreased when systolic dysfunction occurred [2]. However, in infarcted rat hearts, we observed no change in glucose oxidation rate despite manifest systolic dysfunction [15]. For example, hypertensive Dahl saltsensitive rats subjected to a high-fat diet showed decreased cardiac hypertrophy and improved contractile function [26]. Cardiac substrate preference may also be modulated by stimulating glucose utilization directly. Of note, although these approaches improved cardiac glucose oxidation, possible changes in accessory pathways of glucose metabolism such as the pentose phosphate pathway and the hexosamine biosynthetic pathway could also play a role but have not yet been assessed. Finally, the role of cardiac substrate preference remains controversial and warrants further investigations. Recently, the use of metabolomics has revealed profound changes in amino acid metabolism suggesting its role in metabolic remodeling. Interestingly, their levels were negatively correlated with left ventricular ejection fraction [31]. By combining transcriptomic and quantitative targeted metabolomic profiling, Lai et al. Thus, although specific changes in amino acid metabolism are still poorly understood, first data suggest an important role of amino acid metabolism in the regulation of cardiac hypertrophy and contractile function. The increase in this alternative route of pyruvate may account for the mismatch between glycolysis and glucose oxidation that is commonly seen in models of pressure-overload induced cardiac hypertrophy. Of note, this mismatch may also result from increased lactate formation, although this possibility remains to be evaluated in the hypertrophied heart. Hypertrophy-associated anaplerotic changes have also been confirmed in mice with aortic constriction [27] and in hyperthyroid rats [26]. Thus, induction of anaplerotic pathways appears to be a hallmark of metabolic remodeling in cardiac hypertrophy. Therefore, the role of anaplerotic changes particularly in the regulation of cardiac hypertrophy and energy metaboslim remains incompletely understood. This knowledge gap is due in part to the technical challenges inherent in measuring anaplerosis. Perturbations in mitochondrial structure and function may therefore compromise cardiac energetics significantly. Under normal conditions, mitochondrial material is continuously replenished by a process termed mitochondrial biogenesis. Little is known about the regulation of mitochondrial biogenesis in compensated hypertrophy. However, these hearts exhibited increased mitochondrial damage and mitophagy [40]. Therefore, the induction of mitochondrial biogenic signaling could represent a compensatory mechanism triggered by mitochondrial injury and loss. Collectively, although the regulation of mitochondrial biogenesis and its signaling in cardiac hypertrophy and failure is still incompletely understood, available evidence supports the concept that cardiac mitochondria are affected early and undergo progressive remodeling during the development of cardiac hypertrophy and failure. Interestingly, others and we found that mitochondrial respiration in pressureoverloaded hearts initially increased and did not fall until systolic dysfunction developed [2]. Of note, hypertrophied hearts in this study presented mild diastolic dysfunction without changes in left ventricular ejection fraction [40], indicating an early stage of compensated hypertrophy. The failing heart is believed to be subjected to higher levels of free fatty acids, probably as a result of increased lipolysis [20,21]. Autophagy is a highly conserved process by which organelles and large cellular components are degraded. The products of autophagy (amino acids, fatty acids, sugars, and nucleosides) may then be channeled into both energy generating and biosynthesis pathways. Under normal conditions, basal autophagy is crucial by eliminating damaged organelles and misfolded proteins. In states of nutrient deprivation such as starvation or ischemia, autophagic activity is increased, which may support cell function by mobilizing endogenous nutritional sources [61]. Since cell growth requires stimulation of biosynthesis pathways, these data may appear paradoxical at first glance. However, they are supported by earlier studies showing that blunting of protein degradation mediated by the 178 12. Due to the essential role of autophagy in ventricular remodeling, one might expect that inhibiting autophagy may prevent cardiac hypertrophy and failure. However, studies in knockout models with suppressed autophagy have delivered inconsistent results [68,69]. Given the highly complex regulation of autophagy, it is reasonable to assume that specific changes in the induction or targeting of autophagy but not the autophagic flux itself may affect functional outcome. Because both the induction of autophagy and the processing of autophagic products are linked to metabolism, the role of metabolic remodeling in the regulation of autophagy is an attractive target for future studies. Decreased rates of substrate oxidation ex vivo predict the onset of heart failure and contractile dysfunction in rats with pressure overload. Proteomic remodelling of mitochondrial oxidative pathways in pressure overloadinduced heart failure. Activation of the cardiac proteasome during pressure overload promotes ventricular hypertrophy. Pressure-overload-induced heart failure induces a selective reduction in glucose oxidation at physiological afterload. Cardiac fatty acid metabolism is preserved in the compensated hypertrophic rat heart. Compensated cardiac hypertrophy is characterised by a decline in palmitate oxidation. Analysis of metabolic remodeling in compensated left ventricular hypertrophy and heart failure. Furthermore, it involves changes in metabolic pathways that regulate numerous essential cellular processes such as growth, redox homeostasis, and autophagy. Therefore, modulating cardiac metabolism may also affect these critical processes and improve cardiac function by mechanisms beyond the energetic aspect. Cardiac-specific deletion of acetyl CoA carboxylase 2 prevents metabolic remodeling during pressure-overload hypertrophy. Improved hemodynamic function and mechanical efficiency in congestive heart failure with sodium dichloroacetate. Role of pyruvate dehydrogenase inhibition in the development of hypertrophy in the hyperthyroid rat heart: a combined magnetic resonance imaging and hyperpolarized magnetic resonance spectroscopy study. Energy metabolic reprogramming in the hypertrophied and early stage failing heart: a multisystems approach. Recruitment of compensatory pathways to sustain oxidative flux with reduced carnitine palmitoyltransferase I activity characterizes inefficiency in energy metabolism in hypertrophied hearts. Substrate-enzyme competition attenuates upregulated anaplerotic flux through malic enzyme in hypertrophied rat heart and restores triacylglyceride content: attenuating upregulated anaplerosis in hypertrophy. Glucose 6-phosphate dehydrogenase deficiency increases redox stress and moderately accelerates the development of heart failure. Altered glucose and fatty acid oxidation in hearts of the spontaneously hypertensive rat. In vivo alterations in cardiac metabolism and function in the spontaneously hypertensive rat heart. Myocardial infarction in rats causes partial impairment in insulin response associated with reduced fatty acid oxidation and mitochondrial gene expression. Fatty acid transporter levels and palmitate oxidation rate correlate with ejection fraction in the infarcted rat heart. Fatty acid oxidation enzyme gene expression is downregulated in the failing heart. Altered myocardial fatty acid and glucose metabolism in idiopathic dilated cardiomyopathy. Return to the fetal gene program protects the stressed heart: a strong hypothesis. High-fat diet prevents cardiac hy- [27] [28] [29] [30] [31] [32] [33] [34] [35] [36] [37] 180 12. Hyperglycemia-induced mitochondrial superoxide overproduction activates the hexosamine pathway and induces plasminogen activator inhibitor-1 expression by increasing Sp1 glycosylation. O-linked beta-Nacetylglucosamine transferase is indispensable in the failing heart. Mitochondrial proteome remodelling in pressure overload-induced heart failure: the role of mitochondrial oxidative stress. Depressed mitochondrial transcription factors and oxidative capacity in rat failing cardiac and skeletal muscles. Peroxisome proliferator-activated receptor gamma coactivator-1 promotes cardiac mitochondrial biogenesis. Cardiac-specific induction of the transcriptional coactivator peroxisome proliferatoractivated receptor gamma coactivator-1alpha promotes mitochondrial biogenesis and reversible cardiomyopathy in a developmental stage-dependent manner. Effects of long-term vitamin E supplementation on cardiovascular events and cancer: a randomized controlled trial.
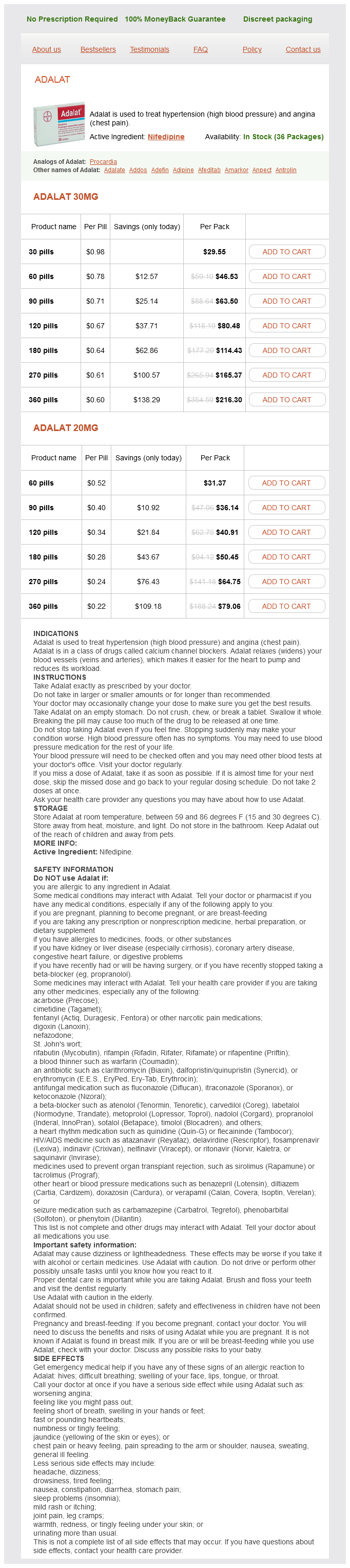
For women nearing menopause prehypertension kidney disease buy 30 mg nifedipine otc, these treatments may be used as a temporizing measure until their own endogenous estrogens decrease naturally blood pressure diastolic low nifedipine 20 mg without prescription. The goal is to decrease the blood supply to the fibroid blood pressure wrist cuff 30 mg nifedipine buy with mastercard, thereby causing ischemic necrosis pulse pressure heart rate cheap 20 mg nifedipine otc, degeneration artery dorsalis pedis 30 mg nifedipine with amex, and reduction in fibroid size. Because the therapy is not specific to a given fibroid, the blood supply to the uterus and/or ovaries can be compromised. The uterine artery, shown here, can be catheterized through a femoral approach under fluoroscopy. As a result, there is decreased blood flow to the fibroids, causing necrosis and devascularization of the fibroids. The technique is typically reserved for premenopausal women who have completed childbearing and wish to retain their uterus. The procedure can be performed in an outpatient setting, but is expensive and not widely available at this time. A myomectomy is the surgical resection of one or more fibroids from the uterine wall. Myomectomy is usually reserved for patients with symptomatic fibroids who wish to preserve their fertility or who choose not to have a hysterectomy. Myomectomies can be performed hysteroscopically, laparoscopically with and without robotic assistance, or abdominally. The primary disadvantage of myomectomy is that fibroids recur in more than 60% of patients in 5 years, and adhesions frequently form that may further complicate pain and infertility. Indications for Surgical Intervention for Uterine Leiomyomas Abnormal uterine bleeding, causing anemia Severe pelvic pain or secondary amenorrhea Uncertainty if mass is a fibroid or another type of tumor Urinary frequency, retention, or hydronephrosis Growth after menopause Recurrent miscarriage or infertility Rapid increase in size Hysterectomy is the definitive treatment for leiomyomas. Vaginal and laparoscopic hysterectomy can be performed for small myomas, and abdominal hysterectomy is generally required for large or multiple myomas. If the ovaries are diseased or if the blood supply has been damaged, then oophorectomy should be performed as well. Otherwise, the ovaries should be preserved in women younger than 65 years with normal-appearing ovaries. Because of the potential for hemorrhage (owing to increased blood supply), surgical intervention should be avoided during pregnancy, although myomectomy or hysterectomy may be necessary at some point after delivery. Women who undergo minimally invasive myomectomies and hysterectomies that utilize power morcellation to remove the specimen have a small risk of spreading an undiagnosed uterine sarcoma-including leiomyosarcomas. Rapid growth of a tumor in postmenopausal women may be a sign of leiomyosarcoma (extremely rare) or other pelvic neoplasia and should be investigated immediately. Low-dose oral contraceptives and hormone replacement therapy at low doses do not appear to pose a risk of recurrence to the patient. These polyps vary in size from millimeters to several centimeters and may be pedunculated or sessile and single or multiple. They are generally within the endometrial cavity but can also prolapse through the endocervical canal into the vagina. Women taking tamoxifen for breast cancer prevention are at risk of developing endometrial polyps, cysts, and cancer. Premenopausal women can present with bleeding between periods (metrorrhagia) but may also have increasingly heavy menses (menorrhagia), heavy irregular bleeding (menometrorrhagia), or postcoital bleeding. Endometrial polyps account for a quarter of all causes of postmenopausal bleeding. Diagnostic Evaluation Pelvic ultrasound, sonohysterogram, and hysteroscopy are the best means of evaluation for the presence, size, and number of polyps, respectively. As with any other etiology for abnormal bleeding, women 45 or older with abnormal bleeding from endometrial polyps should be evaluated with endometrial biopsy prior to removal. For this reason, it is generally recommended that any polyp be removed in postmenopausal patients. It groups endometrial hyperplasia into four groups: simple hyperplasia, complex hyperplasia, simple atypical hyperplasia, and complex atypical hyperplasia (Table 14-6). The groups have a 1%, 3%, 8%, and 29% chance, respectively, of progressing to or having a coexistent endometrial cancer. Unfortunately, this classification system has poor reproducibility and does not account for the difference in malignancy risk of clinical management among the groups. Endometrial proliferation is a normal part of the menstrual cycle that occurs during the follicular (proliferative) estrogen-dominant phase of the cycle. The most common exogenous source is estrogen hormone replacement without progesterone in women with a uterus. In obese women, excess adipose tissue results in increased peripheral conversion of androgens (androstenedione and testosterone) to estrogens (estrone and estradiol) by aromatase in the adipocytes. The changes do not necessarily involve the entire endometrium, but rather may develop focal patches among normal endometrium or coexistent endometrial carcinoma. This includes women with obesity, nulliparity, late menopause, and exogenous estrogen use without progesterone. This is attributed to both the increase in the mass of the endometrium and to the growth of the myometrium in response to continuous estrogen stimulation. Patients may also have stigmata associated with chronic anovulation such as abdominal obesity, acanthosis nigricans, acne, and/or hirsutism. After a history and physical examination, imaging with pelvic ultrasound is typically performed. The pelvic ultrasound may reveal a diffusely thickened endometrial stripe or focal lesion. However, if the sample is inadequate or cannot be obtained owing to patient discomfort or cervical stenosis. The goal of treatment is to control abnormal bleeding and to prevent progression of disease. Benign endometrial hyperplasia (simple and complex hyperplasia without atypia) can be treated medically with progestin therapy. Progestins reverse benign endometrial hyperplasia by counterbalancing the mitogenic effects of estrogen, activating progesterone receptors to stimulate stromal decidualization and thinning of the endometrium. Standardized schedules and dosing for progestin therapy have not been established. Typically, oral medroxyprogesterone acetate (Provera) or megestrol acetate (Megace) is used at doses that will inhibit and eventually reverse benign endometrial hyperplasia. Side effects of progestin therapy can include irregular bleeding, bloating, headaches, irritability, and depression. Micronized vaginal progesterone (Prometrium), levonorgestrel intrauterine system (Mirena), norethindrone (Aygestin), and injectable (Depo-Provera) are alternative treatment modalities. The progestin is usually administered in cyclic or continuous fashion for 3 to 6 months, and then a repeat endometrial biopsy is performed to evaluate for regression of disease. Once the benign endometrial hyperplasia has been treated, preventative therapy should be initiated with regular cyclic or continuous progestin to prevent recurrence. Although unproven, oral and intrauterine progestins have been used with success in this patient population along with serial endometrial sampling. Although the majority of adnexal masses are benign, a chief goal is to rule out malignancy. Postmenopausal women, women with a strong family history of breast and/or ovarian cancer, and women with a hereditary ovarian cancer syndrome are at highest risk for an ovarian cancer. Benign and malignant neoplasms of the ovary are discussed in detail in Chapter 30. Functional cysts of the ovaries result from normal physiologic functioning of the ovaries (Chapter 20) and are divided into follicular cysts and corpus luteum cysts. They arise after failure of a follicle to rupture during the follicular maturation phase of the menstrual cycle. Large follicular cysts can cause a tender palpable ovarian mass and can lead to ovarian torsion when greater than 4 cm and less than 8 cm in size. Most corpus luteum cysts are formed when the corpus luteum fails to regress after 14 days and becomes enlarged (>3 cm) or hemorrhagic (corpus hemorrhagicum). Patients with a ruptured corpus luteum cyst can present with acute pain and signs of hemoperitoneum late in the luteal phase. Theca lutein cysts are large bilateral cysts filled with clear, straw-colored fluid. These ovarian cysts result from stimulation by abnormally high human chorionic gonadotropin. Endometriomas arise from the growth of ectopic endometrial tissue within the ovary. These cysts are also called "chocolate cysts," which comes from the thick brown old blood contained in them. Patients can present with the symptoms of endometriosis such as pelvic pain, dysmenorrhea, dyspareunia, and infertility. The risk is higher in nulliparous women, women with primary infertility or endometriosis, and in women with early menarche or late menopause. The risk of ovarian cancer increases to 5% in a woman with a family history of ovarian cancer in a first degree family member (mother, sister, or daughter). Follicular cysts tend to be asymptomatic and only occasionally cause menstrual disturbances such as prolonged intermenstrual intervals or short cycles. Larger follicular cysts can cause achy pelvic pain, dyspareunia, and ovarian torsion. Corpus luteum cysts may cause local pelvic pain and either amenorrhea or delayed menses. Acute abdominal pain may result from a hemorrhagic corpus luteum cyst, a torsed ovary, or a ruptured follicular cyst. A menstrual and sexual history as well of a family and personal history of breast or ovarian cancer and familial cancer syndromes should be elucidated in patients with adnexal masses. Physical Examination the initial examination of a patient with a cystic adnexal mass or adnexal pain should include an assessment of vital signs, general appearance, along with an abdominal and ingunal lymph node examination. The findings on bimanual pelvic examination vary with the type of cyst, but should include an evaluation of the vulva, vagina, cervix, uterus, and adenexa. Lutein cysts are generally larger than follicular cysts and often feel firmer or more solid on palpation. A ruptured cyst can cause pain on palpation, acute abdominal pain, and rebound tenderness. When an ovarian cyst results in a torsed adnexa, the patient may have an acute abdomen, nausea, and vomiting. Diagnostic Evaluation Laboratory tests should be guided by the findings on history and physical. A urine or serum pregnancy test can rule out normal or abnormal pregnancy, while a complete blood count may provide evidence of an infectious or hemorrhagic process. Screening for gonorrhea and chlamydia and for urinary tract infection should be obtained as indicated. The primary imaging tool for the workup for cystic adnexal masses is the transvaginal pelvic ultrasound. Ultrasonography allows for better characterization of the cyst that can guide the workup and treatment. Table 14-8 and Chapter 30 review the ultrasound findings associated with benign versus malignant cystic adnexal masses. Benign cystic masses tend to be unilateral, <10 cm, and simple in appearance with thin, smooth walls. Some benign complex masses such as endometriomas and dermoid cysts have classic sonographic appearances. Malignancy is suggested by a complex mass greater than 10 cm with mural irregularities, septations, papillary or solid components, internal blood flow, and/or associated ascites. Management of a Cystic Adnexal Mass Age Premenarchal Reproductive Type Any Simple Size of Cyst (cm) >2 cm 5 >5 and 7 >7 Management Surgical evaluation No follow-up necessary Repeat ultrasound in 1 y Further imaging or surgical evaluation if change No follow-up necessary Repeat ultrasound in 612 wk Repeat ultrasound in 612 wk. Because most functional cysts will spontaneously resolve over 60 to 90 days, serial ultrasounds at that interval may be used to check for cyst resolution. These may provide assessment of nearby structures and look for evidence of ascites, lymph node enlargement, and metastatic disease. This chapter also covers the use of other serum tumor markers in the setting of adnexal masses. Urologic and gastrointestinal sources such as ureteral or bladder diverticula, pelvic kidney and diverticular abscess are less common. Treatment Treatment of cystic adnexal masses depends on the age of the patient and the characteristics of the cyst. During this observation period, patients are often started on oral contraceptives. This is not a treatment for existing cysts but rather to suppress ovulation in order to prevent the formation of future cysts. Although there is no absolute cut off for observation based on ovarian size, nearly all simple ovarian cysts are benign and will resolve spontaneously, even those over 10 cm or in postmenopausal women. Given that <1% of simple cysts will be malignant, observation with periodic ultrasound imaging is a reasonable approach in the absence of symptoms or major risk factors. Observation is also indicated for complex masses that are asymptomatic and presumed benign, such as dermoid cysts, endometriomas, and hydrosalpinx. Surgical intervention is indicated in patients who are acutely symptomatic with pain, infection, hemorrhage, or torsion. Surgical removal should be performed if a mass under observation becomes symptomatic or shows growth. Similarly, when possible, an attempt should be made to maximize preservation of ovarian function.
Given the risk of uterine rupture pulse pressure 56 30 mg nifedipine purchase with mastercard, at the very least the patient needs to be expectantly managed with continuous fetal monitoring arteria umbilical unica pdf 20 mg nifedipine order mastercard. The patient labors spontaneously without an epidural but after 4 hours her cervical examination is unchanged jugular pulse pressure discount nifedipine 30 mg buy online. Two hours later the patient is found to be 8 cm dilated blood pressure chart 50 year old male nifedipine 20 mg buy lowest price, 90% effaced arrhythmia in cats discount nifedipine line, and 0 station. Approximately 1 hour later, the nurse calls you to the room because the patient is complaining of severe abdominal pain with and without contractions. Answer D: the most likely explanation for these findings in this clinical scenario is uterine rupture of the prior cesarean scar. The rupture of the scar disrupts uterine blood flow to the placenta, resulting in uteroplacental insufficiency, which in turns causes late decelerations. Severe abdominal pains with loss of station of the fetal head on vaginal examination are classic findings in a uterine rupture, especially when associated with a nonreassuring fetal status on the continuous fetal monitoring. While placental abruption can result in recurrent late decelerations as a result of uteroplacental insufficiency and can occur with a uterine rupture, it is unlikely in this situation as there is minimal bleeding noted. Additionally, loss of station is not generally found on a placental abruption unless it occurs concurrently with uterine rupture. Fetal head compression causes early decelerations, not late decelerations, and does not result in the loss of station on vaginal examination. Umbilical cord compression is not generally associated with pain worse than usual with contractions, causes variable decelerations, and does not cause loss of station of the fetal head. It can result in placental abruption, or if the fetus is delivered through the uterine dehiscence into the abdomen, it can result in significant fetal hypoxic injury because of complete cord compression. Additionally, there is risk for significant maternal blood loss; thus, immediate delivery via cesarean section is imperative. Once the neonate is delivered, the surgeon should then assess the uterine rupture site for the feasibility of repair and to obtain hemostasis. If it cannot be repaired or hemostasis cannot be obtained, peripartum hysterectomy is indicated. While intuitively it is important to stop the oxytocin augmentation when one suspects uterine rupture, expectant management would not be appropriate. An amnioinfusion is not appropriate in this clinical situation, as there is no evidence of cord compression. While there may be uterine tetany as a result of excess oxytocin, once the uterus has dehisced, tocolysis is neither appropriate nor helpful in this situation. Normal labor does not cause significant blood loss with cervical change except in the instance of placenta previa. While patients who labor with a placenta previa can have pain from the contractions and profuse vaginal bleeding, they are not usually hemodynamically unstable nor are they usually in severe pain with a rigid abdomen. Vasa previa can lead to profuse vaginal bleeding if a patient ruptures her membranes and the fetal vessels also rupture, but it does not result in maternal hemodynamic instability. A cervical tear from intercourse can cause significant pain and vaginal bleeding but does not fit with this clinical scenario. Answer C: Typically, when a patient in this scenario presents to the emergency department or obstetrics triage unit, multiple steps are undertaken at the same time. However, the best next step is to start stabilizing the patient and to assess the fetal status. Ultrasound is also important to determine the location of the placenta if there is any concern for a placenta previa. Often it is not necessary at all in the setting of placental abruption as most proceed to emergent cesarean delivery if the fetus has a documented heart rate. Transvaginal ultrasound should come later if the patient stabilizes and needs further assessment of placental location because placenta previa is suspected. Answer A: In the setting of suspected placental abruption, once the fetus is determined to have a heart rate and to be in distress, emergent cesarean delivery is indicated. If delivery is imminent, then the patient can begin pushing, but otherwise one should proceed with emergent cesarean section. A urine drug screen is important because placental abruption frequently occurs in the setting of cocaine abuse and this patient in particular is high risk for cocaine abuse. The patient undergoes delivery with Apgar scores of 1 and 5, at 5 and 10 minutes, respectively. The placenta is removed easily and 500 mL clot follows the delivery of the placenta. Consumptive coagulopathy is commonly associated with placental abruption, particularly in the setting of preeclampsia. It can be fatal if adequate resuscitation is not administered in a timely fashion. It is important to anticipate profound blood loss and coagulopathy with placental abruption. It is also important to follow fibrinogen and to transfuse cryoprecipitate as needed. Acute renal failure as a result of acute tubular necrosis is common in this scenario and usually resolves with adequate resuscitation. It differs from cervical insufficiency, which is a silent, painless dilation, and effacement of the cervix. Both can result in preterm delivery, which is the leading cause of fetal morbidity and mortality in the United States. The incidence of preterm delivery in the United States reached a peak in 2005 to more than 12% of all births but since then has been steadily declining and as of 2014 was 9. Unfortunately, the reason for the rise was predominantly from iatrogenic deliveries, and thus the recent decline has more to do with policy interventions to avoid unindicated, iatrogenic preterm delivery as opposed to medical interventions that have decreased preterm births. Despite this recent decline, large racial and ethnic disparities in preterm birth still exist; for example, as of 2014, African American infants were 50% more likely to be born preterm compared with their Caucasian counterparts. There are three subcategories of preterm birth based on gestational age at the time of delivery: extremely preterm (<28 weeks), very preterm (28 to <32 weeks), and moderate to late preterm (32 to <37 weeks). Morbidity and mortality of preterm infants are dramatically affected by gestational age and birth weight. Long-term complications of prematurity include bronchopulmonary dysplasia and asthma; neurologic disorders, including cerebral palsy, behavioral problems, and learning disabilities; retinopathy of prematurity; and hearing loss. It is difficult to conduct placebo-controlled studies of new tocolytics because most patients and clinicians are unwilling to allow contractions to proceed without some tocolytic therapy. Thus, many of the current trials compare currently used tocolytics with other tocolytics. Because the evidence for which of the tocolytic agents may be the most effective is unclear, institutions and practitioners vary widely in practice. The principal goal of tocolytic therapy is to delay delivery by at least 48 hours. This is because the principal benefit is to allow treatment with steroids to enhance fetal lung maturity and reduce the risk of complications associated with preterm delivery. Prior to 34 weeks of gestation, the advantages of treating with steroids need to be weighed against the risks of prolonging the pregnancy. From 34 to 36 weeks and 6 days, betamethasone has now been shown to be beneficial but is not used with concomitant tocolysis (N Engl J Med. Chorioamnionitis, nonreassuring fetal testing, and significant placental abruption are absolute indications to allow labor to progress and often to hasten delivery. With many other issues, such as maternal disease- particularly preeclampsia or poor placental perfusion-an assessment of the severity of the situation, the precipitous nature of the complication, and the risks from prematurity all contribute to the decision of whether or not to tocolyze. In the case of preterm contractions without cervical change, hydration can often decrease the number and strength of the contractions. For patients who do not respond to hydration or whose cervices are actively changing, a variety of tocolytics may be used. Currently, in the United States, the most commonly used tocolytics are nifedipine and indomethacin. Calcium Channel Blockers Calcium channel blockers decrease the influx of calcium into smooth muscle cells, thereby diminishing uterine contractions. In clinical trials, nifedipine has been the principal drug studied and has been shown to reduce the risk of delivery within 48 hours compared with placebo/no treatment but was not statistically different when compared with other classes of tocolytics. Because nifedipine is a peripheral vasodilator, its main side effects include headaches, flushing, and dizziness. Typically, a 10-mg dose Q 15 minutes is given for the first hour or until contractions have ceased. The optimal dosing of nifedipine, however, has not been established, and so loading and maintenance doses may vary between providers. Nifedipine is contraindicated in women with preload-dependent cardiac lesions and hypotension and should be used with caution in women with left ventricular dysfunction. Also, the concomitant use of nifedipine and magnesium sulfate necessitates caution given their potential synergistic effect that results in respiratory depression. Prostaglandin Inhibitors Prostaglandins increase the intracellular levels of calcium and enhance myometrial gap junction function, thereby increasing myometrial contractions. Thus, they are commonly used to induce labor and to heighten contractions in postpartum patients with uterine atony. Conversely, antiprostaglandin agents are used to inhibit contractions and possibly halt labor. In clinical trials, it has been shown to effectively decrease contractions and forestall labor with minimal maternal side effects. However, it has been associated with a variety of fetal complications, including premature constriction of the ductus arteriosus, pulmonary hypertension, and oligohydramnios secondary to reduced fetal urine output as a result of enhanced vasopressin action and reduced renal blood flow. Furthermore, one study showed an increased risk of necrotizing enterocolitis and intraventricular hemorrhage in extremely premature fetuses that had been exposed to indomethacin within 48 hours of delivery. If indomethacin is used, the amniotic fluid index should be checked before initiating the drug and again after 48 hours, to monitor for development of oligohydramnios. Maternal contraindications to indomethacin include platelet dysfunction, hepatic dysfunction, gastrointestinal ulcerative disease, renal dysfunction, and asthma. Indomethacin is given orally as a 50-mg loading dose followed by 25 mg every 6 hours for 48 hours. Magnesium Sulfate Magnesium decreases uterine tone and contractions by acting as a calcium antagonist and a membrane stabilizer. Although magnesium can stop contractions, in small placebo-controlled trials, it has not been shown to change gestational age of delivery. In larger trials, the efficacy of magnesium did not vary significantly from that of -mimetics. At toxic levels of magnesium (>10 mg/dL), respiratory depression, hypoxia, and cardiac arrest have been seen. Generally, magnesium sulfate should be loaded as a 6-g bolus over 20 minutes, and then maintained at a 2 g/hour continuous infusion. A slower infusion should be used in the case of renal insufficiency because magnesium is cleared via the kidneys. Subcutaneous terbutaline is still used to acutely stop contractions in the setting of uterine hypertonicity leading to an abnormal fetal heart tracing. Although they have shown to decrease uterine myometrial contractions, clinical studies have been small and have not demonstrated an improvement in outcomes. The diagnosis is made by obtaining a history of leaking vaginal fluid, pooling on speculum examination, and positive nitrazine and fern tests. If these tests are equivocal, an ultrasound can be performed to examine the level of amniotic fluid. If the diagnosis is still unconfirmed, an amniocentesis dye test can be performed by injecting a dye via amniocentesis and observing whether or not the dye leaks into the vagina. This is also known as the tampon test because the dye is usually identified by its absorption into a tampon. Up to this point, the risk of prematurity drives management, whereas after this point, the risk of infection motivates delivery. With that said, in the setting of intrauterine infection, acute placental abruption, or nonreassuring fetal testing, expeditious delivery regardless of gestational age is appropriate. However, at many institutions, tocolysis is used for 48 hours, particularly at earlier gestational ages, in order to gain time to administer a course of corticosteroids. Some patients may elect to bear the risk of increased infection to await the onset of spontaneous labor. The three "Ps"-pelvis, passenger, and power-are primarily responsible for a vaginal delivery. Common measurements of the pelvis include those of the pelvic inlet, the midpelvis, and the pelvic outlet. The face and base are composed of fused bones that do not change during labor; however, the bones of the vault are not fused and can undergo molding to conform to the maternal pelvis. The vault is composed of five bones: two frontal, two parietal, and one occipital. The spaces between the bones are known as sutures; the two places where the sutures intersect are the anterior and posterior fontanelles. How the fetal head presents to the maternal pelvis is important in accomplishing a vaginal delivery. There is great variation in the diameter of the skull at various levels and with various inclinations. When the fetal skull is properly flexed, the suboccipitobregmatic diameter presenting to the pelvis averages 9. When the sagittal suture is not located midline in the pelvis (asynclitism), the diameter of the skull being accommodated is effectively increased. Persistent breech presentation is also associated with placenta previa and fetal anomalies. Complications of a vaginal breech delivery include prolapsed cord and entrapment of the head. The frank breech has flexed hips and extended knees, and thus the feet are near the fetal head. The complete breech has flexed hips, but one or both knees are flexed as well, with at least one foot near the breech.
Effective nifedipine 30 mg. "Magic Potion" Tea Helps Control Blood Pressure (Proof).
References
- Costa G, Di Milia L. Aging and shift work: a complex problem to face. Chronobiol Int 2008;25:165-81.
- Veatch RM: Patient, heal thyself: how new medicine puts the patient in charge, 2009, Oxford University Press. Veatch RM: The patient-physician relation: the patient as partner, 1991, Indiana University Press. Weinstein ND: Optimism biases about personal risks, Science 246:1232-1233, 1989.
- Cavanagh NP, Lake BD, McMeniman P, et al. Congenital fibre type disproportion myopathy. A histological diagnosis with an uncertain clinical outlook. Arch Dis Child. 1979;54(10):735-743.
- Wu, J., Li, B., Li, W., Jiang, Y., Liang, J., Zhong, C. Laparoscopic vaginal reconstruction using a ileal segment. Int J Obstet Gynecol 2009;107:258-261.
- Adams BD, McHugh KA, Bryson SA, et al: The law of unintended consequences: the Joint Commission regulations and the digital rectal examination. Ann Emerg Med 51:197-201, 2008.
- Albrektsson T, Gottlow J, Meirelles L, et al. Survival of Nobel Direct implants: an analysis of 550 consecutively placed implants at 18 different clinical centers. Clin Implant Dent Relat Res 2007;9:65-70.