Zyrtec
Zyrtec 10mg
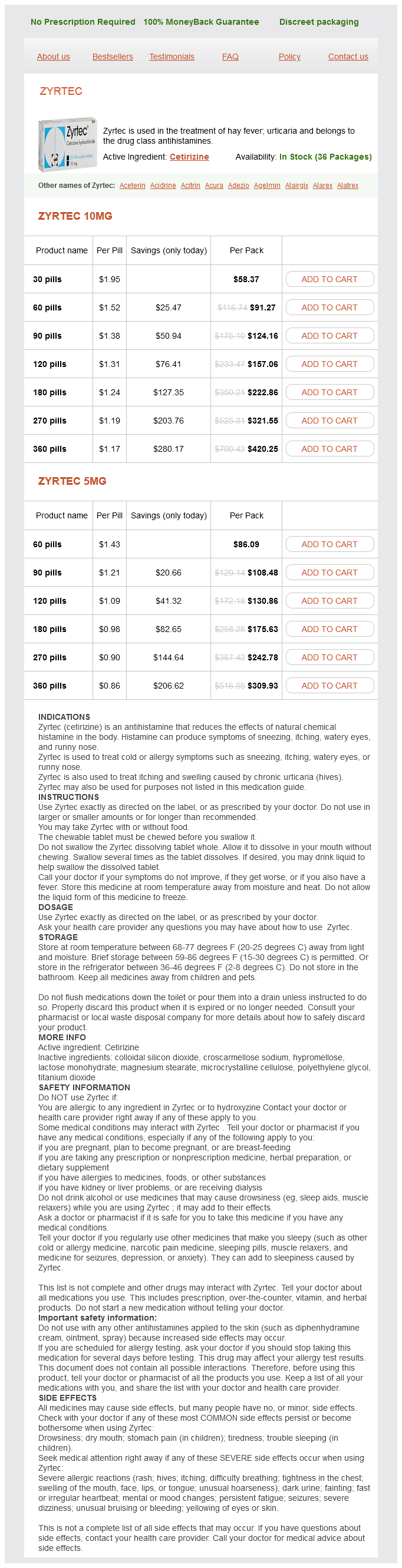
- 30 pills - $58.37
- 60 pills - $91.27
- 90 pills - $124.16
- 120 pills - $157.06
- 180 pills - $222.86
- 270 pills - $321.55
- 360 pills - $420.25
Zyrtec 5mg
- 60 pills - $86.09
- 90 pills - $108.48
- 120 pills - $130.86
- 180 pills - $175.63
- 270 pills - $242.78
- 360 pills - $309.93
Zyrtec dosages: 10 mg, 5 mg
Zyrtec packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 808
Only $0.91 per item
Description
Thus girls present in infancy or childhood with hypertension allergy treatment in toddlers zyrtec 5 mg buy otc, hypokalemia, acne, hirsutism, and virilization; whereas boys present with pseudoprecocious puberty. After appropriate diagnosis (typically by determination of levels of steroid precursors in serum), patients with congenital adrenal hyperplasia receive supplementation with glucocorticoids, which suppress corticotropin secretion, and reduction of the signs and symptoms of mineralocorticoid excess. Very rare causes of mineralocorticoid excess include deoxycorticosterone-producing tumors (which are usually quite large and often malignant), primary cortisol resistance, or 11-hydroxysteroid dehydrogenase deficiency (of which approximately 50 cases worldwide are congenital; most are acquired and associated with imported licorice or licorice-flavored chewing tobacco). The probability of renovascular hypertension can be calculated, based on clinical characteristics in a given patient, which eliminates the need for a screening test in most cases. The choice among the several screening tests for renovascular hypertension is usually based on patient and physician preference, local expertise, and a favorable decision about prior authorization for the test from insurance companies, which has become less common since the publication of several outcome studies that showed no significant benefit to renal angioplasty (usually with stenting) over medical management in atherosclerotic renal artery disease. The clinical presentation of patients with these tumors is quite variable, as symptoms may occur constantly or in paroxysms. The classical triad of headache, sweating attacks, and hypertension was said to be present in 95% of patients in one large French series, but most centers report having to see more than 100 such patients on referral before one is positively diagnosed. Some heredofamilial conditions that include pheochromocytoma have characteristic physical signs. There seem to be more "exceptions" to pheochromocytoma than with many other conditions: approximately 10% of such tumors are extraadrenal, multiple or bilateral, recurrent (after surgical extirpation), discovered as "incidentalomas," or in children; more than 10% are likely heredofamilial or metastatic at presentation (and both of these have increased in the last 30 years). Although approximately 90% of pheochromocytomas are found in or in close proximity to an adrenal gland, paragangliomas can occur anywhere along the sympathetic ganglia, but most commonly in or near the organ of Zuckerkandl (at the aortic bifurcation) or near the bladder (which gives rise to rather unusual symptoms of "micturition headache," syncope, or the like). Both of these conditions can be diagnosed using genetic screening, although this is often more fruitful for screening family members after an index case has been identified. Availability of genetic testing for these mutations has made disease surveillance for those who carry these genes (typically relatives of index cases) much simpler. Measurements of plasma-free or urinary fractionated metanephrines are most commonly recommended, but a wide variety of factors are known to produce both false-positive and false-negative results. In some centers, plasma-free metanephrines (which provide a very brief "snapshot" of catecholamine production and metabolism) can be assayed quickly and accurately; in others, integration of catecholamine production and metabolism over a longer time period is less expensively performed using urinary collections. Pharmacologic testing for pheochromocytoma is occasionally used in equivocal cases; clonidine suppression testing is usually preferred over glucagon stimulation testing, although most managed care organizations recommend a repeat plasma or urinary collection 6 or more months after the initial evaluation. To improve cost-effectiveness and reduce radiation exposure, imaging studies for pheochromocytoma and related tumors are generally not obtained until after biochemical evidence of catecholamine overproduction is obtained. In this setting the higher resolution available from computed tomographic scans (with thin cuts of the adrenals) outweighs the more specific finding of a T2-weighted "bright spot" on magnetic resonance imaging. The role of genetic testing in routine care of patients with pheochromocytoma is evolving; current guidelines recommend a shared decision-making process, often involving more family members than just the index patient.
Disodium ethylenediamine tetraacetic acid (Edta). Zyrtec.
- Treating coronary heart disease (CHD) or peripheral arterial occlusive disease.
- What other names is Edta known by?
- Emergency treatment of life-threatening high calcium levels (hypercalcemia).Treating heart rhythm problems caused by drugs such as digoxin (Lanoxin).
- Dosing considerations for Edta.
- How does Edta work?
- Are there any interactions with medications?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96988
At least two studies have examined the use of two daily exchanges with icodextrin and demonstrated a higher ultrafiltration volume and improvement in other clinically relevant parameters salicylate allergy symptoms uk zyrtec 5 mg purchase with mastercard. Hybrid solutions containing both icodextrin and glucose have also been tested and shown to have substantially higher ultrafiltration volumes; however, no hybrid solutions are commercially available. In addition, glucometers that use glucose dehydrogenase pyrroloquinoline quinone overestimate the blood glucose levels secondary to the accumulation of maltose. Episodes of aseptic peritonitis have also been reported in patients treated with icodextrin. This complication has been traced to the presence of peptidoglycan in the solution from hydrolysis of corn starch, and the problem has been substantially minimized with changes in manufacturing processes such that the commercially available solution does not have any detectable peptidoglycan. A large number of clinical trials have examined the potential clinical benefits with such biocompatible solutions, but the evidence base consists of studies with heterogeneous results. Nevertheless, there is no evidence for harm with the use of this solution, and the decision to use it is dictated by both the availability and the cost of the solution. Continuous regimens are the ones in which there is intraperitoneal dialysate 24 hours a day, 7 days a week. Similarly, patients with faster peritoneal solute transfer rates (fast or high transporters) could benefit with shorter nighttime dwells to optimize daily ultrafiltration. There is no evidence for better preservation of structural or functional integrity of the peritoneum in humans treated with a bicarbonate-based solution. However, this solution results in a more complete correction of metabolic acidosis and reduces infusion pain. An observational study has demonstrated a lower risk for death in patients treated with this solution,143 but no clinical trial has validated this finding. The use of this solution, thus, is dictated by its availability and cost, as there is no clear-cut evidence for any clinically meaningful benefit. Central to such glucose-sparing regimens is substitution of one glucose-based exchange with icodextrin for the long dwell. Although clinical indicators should not be ignored, therapeutic decisions should not be based solely on them. In addition, its volume of distribution is the total body water, it easily diffuses across the dialysis membrane, and it is easy to measure. Peritoneal Kt is calculated by collecting a 24-hour amount of effluent dialysate and determining its urea concentration (Durea); this in turn is divided by the plasma urea concentration (D/Purea). To compare clearance values among patients, these values are normalized to a function of patient size: For urea, the metric is typically the volume of urea distribution (V).
Specifications/Details
Compared to the control diet allergy symptoms milk protein order 5 mg zyrtec with mastercard, the mean reductions in systolic and diastolic blood pressures associated with the combination diet were 5. For the 133 subjects who were hypertensive, the results were more pronounced; systolic and diastolic pressures were lowered by 11. This is recommended because a diet restricted in potassium and sodium is difficult to achieve. First, this amount of dietary protein is not needed by all subjects as some will require less than this amount and others require more. In adults, eating more than this amount does not improve body protein stores because the catabolic pathways described earlier stimulate losses of protein stores. Patients with Nephrotic Syndrome Patients with hypercholesterolemia, edema, and more than 3 g urinary protein/day. Similarly, these adaptive metabolic responses occur when the diet is restricted to only 0. There is a significant correlation between the amount of dietary protein and leucine oxidation during fasting and feeding, showing the adaptive response to dietary protein changes. Notably, the defect cannot be corrected by giving nephrotic patients a protein-rich diet. Unfortunately, some of the published studies are of low methodologic quality because they were retrospective studies with only a small number of patients or serious design flaws. Instead, outcomes in reported trials were based on estimating differences in changes in serum creatinine levels or the degree of proteinuria. There are different types of phosphate anions, and the proportions of these anions depend critically on the blood pH and other factors, making the interpretation of the plasma phosphates complex. Because of the marked influence of pH on the different types of phosphates, clinical laboratories do not report phosphate concentrations but report the serum concentration of phosphorus, which represents the concentration of all types of phosphates. Therefore, patients and physicians concentrate on regulating the amount of phosphorus in the diet, even though all physiologically important reactions are based on phosphate metabolism. The intake of phosphates is linked to dietary protein by a predictable relationship-approximately 1 g of protein contains 13 mg of phosphate-and, consequently, variations in the amount of protein eaten will predictably change phosphorus intake. The serum phosphorus level, therefore, is influenced by the amount of protein in the diet as well as processes that regulate phosphate metabolism, including the intestinal absorption of dietary phosphates, excretion of phosphates by renal tubules, and changes in bone metabolism. This finding suggests that phosphate retention is not a prominent reason for the development of secondary hyperparathyroidism (see Chapters 55), but there are flaws in this suggestion. Nevertheless, it is generally agreed that the pathophysiology of hyperparathyroidism depends on phosphate retention due to lost kidney function.
Syndromes
- Abdominal aortic aneurysm
- Intestine (mesenteric artery aneurysm)
- Have a family history of thyroid cancer
- Tyrosine
- You have sudden, severe hearing loss or ringing in the ears (tinnitus)
- Stroke
- Have you had urinary or kidney problems in the past, or recently had surgery or an injury?
Related Products
Usage: b.i.d.
Additional information:
9 of 10
Votes: 243 votes
Total customer reviews: 243
Customer Reviews
Xardas, 21 years: These anomalies include vesicoureteral reflux (25%), ureteropelvic junction obstruction (11%), and ureterovesical junction obstruction (11%). For membrane filtration plasmapheresis, the use of standard unfractionated heparin is preferred, and the required dose of heparin is about twice that needed for hemodialysis because a significant amount of infused heparin is removed along with the plasma. The primary patency is shorter after angioplasty of central vein stenosis as compared with other stenotic locations.
Lee, 56 years: Schepers E, Meert N, Glorieux G, et al: p-Cresylsulphate, the main in vivo metabolite of p-cresol, activates leucocyte free radical production. Chandak P, Kessaris N, Durkan A, et al: Is laparoscopic donation safe for paediatric recipients The precalyceal canalicular ectasia may involve one or more renal papillae in one or both kidneys, and the lesions are bilateral in 70% of cases.
Nasib, 31 years: Sakemi T, Ohtsuka N, Yoshiyuki T, et al: Testosterone does not eliminate the attenuating effect of estrogen on progressive glomerular injury in estrogen-treated hypercholesterolemic male Imai rats. The distinction between the two is important because the management approach is substantially different. They allow differentiation of falciparum from non-falciparum malarias, but results can remain positive for several weeks after acute infection.
Sven, 55 years: Treatment requires hydration and urine alkalinization with sodium bicarbonate to increase djenkolic acid solubility. Xu G, Liu A, Liu X: Aldosterone induces collagen synthesis via activation of extracellular signal-regulated kinase 1 and 2 in renal proximal tubules. Yoshida Y, Kawamura T, Ikoma M, et al: Effects of antihypertensive drugs on glomerular morphology.
Bradley, 52 years: Allograft rejection because of red blood cell type mismatching can be readily prevented by routine blood typing before transplantation. Loss of a part or all of rigid catheter after manipulation of a poorly functioning rigid catheter has been reported. Ito S, Kamei K, Ogura M, et al: Survey of rituximab treatment for childhood-onset refractory nephrotic syndrome.
Peer, 35 years: The usual daily dose is 180 to 480 mg, with an elimination halflife of up to 10 hours. The resistive index provides an estimate of the relative flow velocities in diastole and systole. In Mayatepek E, editor: Pädiatrie, Munich, 2007, Elsevier/Urban & Fischer, pp 683-733.
Contact
0673406227
dppsmyanmar@gmail.com