Zofran
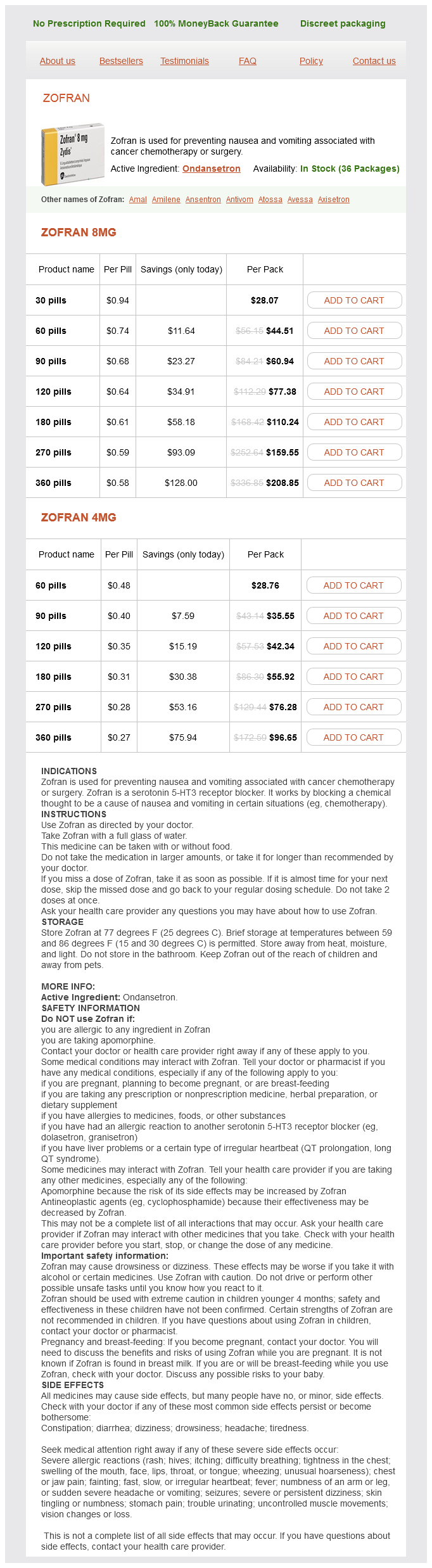
Zofran 8mg
- 30 pills - $28.07
- 60 pills - $44.51
- 90 pills - $60.94
- 120 pills - $77.38
- 180 pills - $110.24
- 270 pills - $159.55
- 360 pills - $208.85
Zofran 4mg
- 60 pills - $28.76
- 90 pills - $35.55
- 120 pills - $42.34
- 180 pills - $55.92
- 270 pills - $76.28
- 360 pills - $96.65
Zofran dosages: 8 mg, 4 mg
Zofran packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 589
Only $0.29 per item
Description
Staff should have competencies in monitoring symptoms after conception zofran 8 mg order visa, interpretation and response to the acute deterioration. Medium score group: urgent call to the primary medical team simultaneous call to personnel with competencies in acute illness. These competencies should include assessment of the critically ill patient, advanced airway management and resuscitation skills. Multiple parameter systems are more complex but allow for better monitoring of clinical progress and for a graded response strategy, but may lack reproducibility. Whatever track-and-trigger system is used locally, escalation policies should be agreed as well as follow-up of the recognized deterioration. To support this, some institutions use specialized response teams or critical care outreach that can be contacted if a patient deteriorates. Physiology of oxygen Blood oxygen content (CaO2) is the sum of the oxygen bound to haemoglobin (Hb-O2) and the oxygen dissolved in plasma: 1 g of haemoglobin is able to bind a maximum of 1. The amount of oxygen dissolved in plasma is so small that, for most purposes, it can be almost ignored. Advanced haemodynamic monitoring has established itself as an invaluable tool to guide therapy in the critically ill patient. And, indeed, haemodynamic monitoring has been shown to improve outcome in a variety of settings. This section will discuss some elements of advanced haemodynamic monitoring and the underlying cardiovascular physiology. After initial promising results, other authors were not able to confirm this hypothesis and the concept has been abandoned these days. Moreover, evidence has emerged recently that, rather than a decrease in overall oxygen delivery, microcirculatory abnormalities and an inability to extract oxygen (dysoxia) seem to prevail in critical illness. Note that the dicrotic notch in a peripheral arterial wave is thought to be the pressure wave reflected peripherally rather than the closure of the aortic valve. In addition, frequent arterial blood gas analyses are often necessary in critically ill patients who receive mechanical ventilation. The radial, femoral and brachial arteries are the most commonly used sites for insertion. The arterial pressure is transduced via a short extension of rigid manometer tubing. A marked respiratory swing of the arterial wave can signify hypovolaemia, especially in a ventilated patient. Central and mixed venous oxygen saturation Central venous oxygen saturation can be measured from blood taken from the superior vena cava.
True Bay (Sweet Bay). Zofran.
- Cancer, dandruff, and relieving gas.
- What is Sweet Bay?
- Are there safety concerns?
- Are there any interactions with medications?
- Dosing considerations for Sweet Bay.
- How does Sweet Bay work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96674
Traumatic subarachnoid haemorrhage Traumatic subarachnoid haemorrhage is blood in the subarachnoid space following trauma medicine to stop diarrhea 8 mg zofran purchase free shipping, and frequently occurs in moderate or severe traumatic brain injury and is related to worse outcome at time of discharge. The presence of traumatic subarachnoid haemorrhage appears to be associated with worse vocational outcome in survivors of moderate or severe traumatic brain injury. As such, the presence of traumatic subarachnoid haemorrhage appears to have predictive value with respect to outcome. Traumatic intracerebral haematoma Traumatic intracerebral haematoma often occurs in addition to acute subdural haematoma or contusion. The difference between cerebral contusion and traumatic intracerebral haematoma is arbitrary. It can happen when a blood clot obstructs the fourth ventricle or the cerebral aqueduct. More often unilateral hydrocephalus follows subfalcine brain hernia owing to obstruction of the third ventricle. Concussion Concussion is transient loss of consciousness following nonpenetrating closed head injury without gross or microscopic brain damage. Concussion is divided into three grades as follows: Grade 1 No loss of consciousness; confusion without amnesia. Pathophysiology of head injuries 339 occur: scalp lacerations, scalp haematomas, skull fractures, cranial nerve injuries, vascular injuries and spinal injuries. Basilar and simple linear skull fractures do not require specific treatment but they could indicate serious underlying brain injury. Compound skull fractures by definition are contaminated and require wound lavage, primary closure and antibiotic treatment for 7 days according to local antibiotic policy. Depressed skull fractures on the other hand may need treatment if they are compound, depressed more than the thickness of the skull or cosmetically unacceptable except when they overly venous sinuses. Scalp lacerations the extent of scalp lacerations does not indicate the severity of brain injury. However, they need to be treated promptly to stop blood loss and to make sure that there is no associated depressed skull fracture. The scalp has five layers: S for skin; C for connective tissue where the blood vessels and nerves are located, hence the blood vessels are kept open and lead to excessive blood loss unless the bleeding is stopped by compression; A for aponeurosis that keeps the scalp stretched; the aponeurosis must be closed when suturing scalp wounds to prevent stretching of the scar; L for loose areolar tissue; and P is for pericranium. Scalp lacerations must be cleansed and closed, making sure the aponeurosis is approximated to prevent the edges from retraction and widening the scar. Local anaesthesia, to be effective, must be injected in the connective tissue layer above the aponeurosis. This often occurs in association with skull base fractures involving the anterior cranial fossa, sphenoid or temporal bones. Prophylactic antibiotics are not indicated here because they merely change the type of organism rather than prevent meningitis. Cephalohaematomas Haematomas of the scalp are not uncommon and do not need specific treatment.
Specifications/Details
In comparison with open repair medications mothers milk thomas hale generic zofran 8 mg, studies have shown a significant decrease in mortality, blood loss, transfusion requirements, paraplegia rates, operating theatre times and length of stay. Endoleaks also occur in 015% of patients and may require additional intervention. The majority are type I endoleaks; this is likely to be related to the technical difficulty in achieving a good proximal seal in the aortic arch. The majority of type I leaks are diagnosed at the time of the original procedure and treated. However, long-term outcomes are unknown and several studies have demonstrated an increased need for secondary interventions among thoracic endovascular aortic repair patients compared with those undergoing open repair. Penetrating thoracic aortic injuries Injuries to the thoracic aorta and great vessels are more commonly due to penetrating mechanisms. Those patients presenting with initial haemodynamic instability and a penetrating wound to the chest require urgent thoracotomy. Patients with transthoracic or transmediastinal gunshot wounds are at risk for vascular, aerodigestive and spinal injuries. Proximal and distal control may require cross-clamping of the descending aorta, with the associated risk of spinal cord ischaemia. Partial bypass techniques have greatly improved over the past several years and should be used within the trauma setting whenever practical. Primary repair of the injury should be attempted when feasible, but intercostal vessels should not be sacrificed to gain mobility owing to the increased risk of spinal cord ischaemia. Dacron interposition grafts can be used if defects are too large for primary repair. In patients with severe physiological derangement, temporary intravascular shunts may be used as a damage control technique. Chest tubes, nasogastric tubes and commercially prepared vascular shunts can all be used depending on the diameter of the injured vessel. The shunts should be secured proximally and distally with silk ties or umbilical tape. Patency appears to be adequate without the use of systemic heparinization, although maximum dwell times are unknown. Blunt cardiac injury can be divided into abnormalities of conduction and those of structure. The most common clinically significant electrical disorders are tachyarrhythmias, of which atrial fibrillation is the most likely. Haemodynamically significant arrhythmias are rare and treatment is similar to arrhythmias of nontraumatic aetiology with medications or cardioversion. Structural lesions include blunt cardiac rupture, valvular or papillary muscle rupture, coronary artery injury and myocardial contusion. Structural lesions are best diagnosed with echocardiography, which has an excellent sensitivity and specificity. Few patients with blunt cardiac rupture remain alive long enough to present to the hospital.
Syndromes
- Heart surgery
- Hydrocephalus (fluid collecting in the skull)
- Abnormal liver function test results
- Burns
- Uncontrolled diabetes
- Chronic liver damage and an enlarged spleen
- A closed head injury means you received a hard blow to the head from striking an object, but the object did not break the skull.
- 1 - 3 years: 0.5 mg/day
Related Products
Usage: ut dict.
Additional information:
9 of 10
Votes: 109 votes
Total customer reviews: 109
Customer Reviews
Silas, 65 years: Eventration of diaphragm Anomalous congenital development of the diaphragm or its innervation may result in unilateral elevation of the diaphragm. Cortisol has a wide range of physiological actions involving fat, carbohydrate and protein metabolism and is subject to a specific diurnal variation in synthesis and production, with highest levels being achieved early in the morning and lowest levels at night.
Grompel, 49 years: An appropriate physiological response to the stress of surgical intervention is to increase cardiac output. Management of splenic trauma has undergone a revolution since the 1990s as appreciation of the dangers of abdominal sepsis and overwhelming postsplenectomy sepsis has risen.
Trano, 35 years: This arcade gives off delicate branches to the lesser curve but most of its bigger branches pierce the seromuscular coat anteriorly and posteriorly to join the submucosal vascular plexus of the stomach. They tend to occur Warts Warts are exceedingly common, and it is estimated that about 10% of all individuals are affected, usually teenagers, but they may occur at any age.
Uruk, 30 years: Specific bacterial infections of surgical importance 209 of the dead muscle completes the pathological process with the production of the characteristic fishy odour and the greenishblack appearance of the established disease. The more usual sliding hernia involving the colon forms a large inguinal mass and is often irreducible by the time of diagnosis.
Contact
0673406227
dppsmyanmar@gmail.com