Urispas
Urispas 200mg
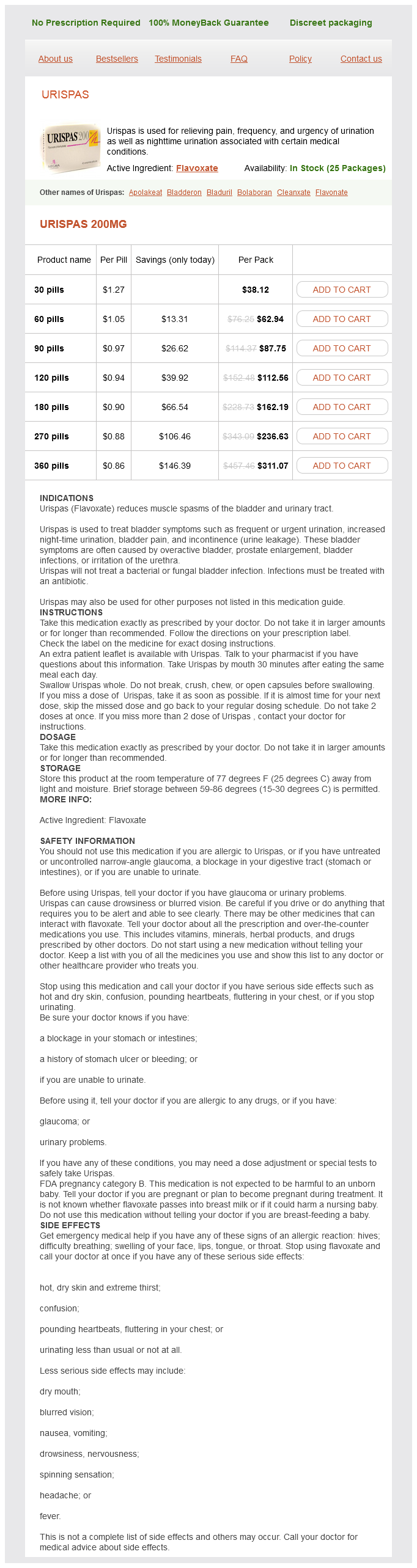
- 30 pills - $38.12
- 60 pills - $62.94
- 90 pills - $87.75
- 120 pills - $112.56
- 180 pills - $162.19
- 270 pills - $236.63
- 360 pills - $311.07
Urispas dosages: 200 mg
Urispas packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 625
Only $0.92 per item
Description
Interdisciplinary teams combining chemical spasms near ribs 200 mg urispas purchase with visa, biological, genetics, and informatics expertise contribute to shorten the timeframe required for drug discovery processes. Moreover, emerging technologies coupled with new high-resolution and powerful instrumentation will help speed up this process, thereby tackling the challenge represented by the discovery and subsequent exploitation of the treasure concealed in the nature. The situation significantly improved when penicillin and other classes of antibiotics were discovered and used to treat infectious diseases. However, almost as soon as antibacterial drugs were introduced in clinics, bacterial resistance spread [1, 2]. Antibiotic resistance can be defined taking into account the pharmacokinetic and pharmacodynamic criteria to determine values above which a therapeutically useful concentration is difficult to obtain. From a medical, social, and economical viewpoint, resistant bacteria, becoming commonplace in healthcare institutions, often result in treatment failure and this implies an added burden on healthcare costs [3]. In addition, resistant bacteria may also spread and become broader infection-control problems, not only within healthcare institutions but in communities as well [4, 5]. From a biological and microbiological viewpoint, antibacterial drug resistance is a fascinating aspect of molecular evolution and selection of fine mechanisms that allow survival under unfavorable circumstances. In particular, under the selective pressure of antibiotics, bacteria evolve and spread resistance mechanisms that become common to pathogenic and nonpathogenic strains. The resistome includes the totality of those genetic elements whose function is to counteract toxic effects of antibiotic drugs. Furthermore, the resistome also comprises the collection of genes, called protoresistance genes, which have the Antibiotics: Targets, Mechanisms and Resistance, First Edition. Many resistance genes have been isolated from clinically relevant strains and from the vast reservoir of environmental nonpathogenic organisms. Antibiotic-producing environmental bacteria most probably are the original source of many resistance enzymes, reflecting a continuous evolutionary pressure where antibiotic biosynthesis and resistance coevolve [7, 8]. In fact, in soil environments, evolutionary pressure promotes the development and spread of resistance genes among pathogenic and nonpathogenic bacterial genera. This hypothesis is supported by the presence of resistance elements in antibiotic-producing bacteria that have orthologs in clinical isolates [912]. Anyway, antibiotic-producing bacteria could not be the sole source of resistance genes. In fact, bacterial genomes contain an unexpected number of genes encoding putative resistance proteins [1315], which could have originated through amplification and random mutation of genes not originally involved in antibiotic resistance, [16]. Primary sequence analysis of resistance proteins, determination of their molecular mechanisms, and three-dimensional structures revealed homologies to known metabolic and signaling enzymes with no antibiotic-resistance activity [7]. Therefore, it is possible that resistance genes originally derived from elements having other metabolic functions, similar to housekeeping genes encoding enzymes with modest and fortuitous resistance properties, evolved into resistance enzymes as a result of selective pressure of antibiotic exposure. The fact that resistance genes are so widespread in the environment and that even resistance to synthetic antibiotics can be readily selected reveals the plastic nature of the link between molecular evolution and resistome, whose origins may predate the actual antibiotic era [17].
D-Alpha-Tocopheryl (Vitamin E). Urispas.
- Helping some heart medications called "nitrates" work better.
- Prostate cancer prevention.
- How does Vitamin E work?
- Helping to treat kidney problems in children (glomerulosclerosis).
- Chemotherapy-related nerve damage. Taking vitamin E before and after treatment with cisplatin chemotherapy might reduce the chance of getting nerve damage.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96917
In addition spasms and cramps buy discount urispas 200 mg online, the emotional burden to parents and families with preterm children in the immediate neonatal period and their overall quality of life through childhood, adolescence, and adulthood are more difficult to measure, but are nonetheless present. T1-weighted and T2-weighted images provide information on macrostructure of the brain, including anatomy, morphology, and volume. It usually appears in the zone of periventricular crossroads of pathways,54 an important anatomic localization relevant for proper ingrowth, outgrowth, and path selection of axonal fibers. Additional findings from many of these studies are that severity of white matter abnormalities is proportionally related to the severity of impairment. Moderate to severe white matter injury was defined using the criteria described by Woodward and colleagues13 taking into account extent of white matter signal abnormality (B, C, arrows; E, arrow), periventricular leukomalacia (E, F, arrows) with periventricular white matter volume loss and dilatation of ventricles (E, asymmetric size of ventricles). Cerebellar hemorrhage is usually unilateral and associated with supratentorial lesions, leading to possible cerebellar atrophy with time. Cerebellar infarction is thought be secondary to general ischemia or to a vaso-occlusive event again leading to parenchymal destruction. Note the different imaging characteristics of white matter injury located in proximity of ventricles. At term-equivalent scan, areas of low T2 signal intensity (F, arrowhead) indicate hemorrhage in the ventricular zone and ganglionic eminence (germinal matrix). The clinical examinations in infancy, early childhood, and at school age revealed persistent right-sided hemiplegia. In addition to motor function, the cerebellum is purported to play a role in a range of other important functions in children, such as cognition, learning, and behavior,7073 and is related to neurodevelopmental sequelae. Clinical report at 13 months after birth (corrected age) revealed delayed psychomotor development. The study assessed for white matter signal intensity changes, hemorrhagic lesions, and cystic lesions in its score of severity. Woodward and colleagues13 described and used a more comprehensive scoring system to define brain abnormalities in preterm infants near term age and related them to neurodevelopmental outcomes. The development and use of more comprehensive and standardized evaluation criteria will likely lead to improvements in the predictive value of neurodevelopmental outcomes. Major destructive lesions, including cerebellar hemorrhage, were related to poorer neurodevelopmental outcomes in early scans. These strategies are described later, and the published neonatal outcome data are available. It allows the measurement of the volume of specific brain structures, including the cortical and subcortical regions, cerebellum, and hippocampus. Appearance of cortical convolutions follows the spatiotemporal schedule and is indirect marker of spatiotemporal and gender differences in brain maturation. Dubois and colleagues105 calculated the sulcation index at birth in 2 groups: children born prematurely with moderate white matter Neuroimaging in Preterm Neonates 271 injury and prematurely born children without signs of white matter injury. Their results showed that children born prematurely with evidence of moderate white matter injury at birth have increased sulcation in the areas of the central sulcus and frontal lobe indicating an alteration of subsequent cortical development, probably caused by similar mechanisms involved in fetal white matter lesionassociated polymicrogyria.
Specifications/Details
If no bacterium is cultured the antibacterial can be continued or stopped on clinical grounds muscle relaxant usage discount 200 mg urispas overnight delivery. Summary of antibacterial therapy If treating a patient suspected of suffering from a notifiable disease, the consultant in communicable disease control should be informed (see p. Antibacterial not usually indicated Campylobacter enteritis Frequently self-limiting; treat if immunocompromised or if severe infection. Clarithromycin1 Alternative, ciprofloxacin Strains with decreased sensitivity to ciprofloxacin isolated frequently Salmonella (non-typhoid) Treat invasive or severe infection. Do not treat less severe infection unless there is a risk of developing invasive infection. Ciprofloxacin or cefotaxime Shigellosis Antibacterial not indicated for mild cases. Ciprofloxacin or azithromycin Alternatives if micro-organism sensitive, amoxicillin or trimethoprim 1. Cefotaxime1 Azithromycin may be an alternative in mild or moderate disease caused by multiple-antibacterial-resistant organisms. Amoxicillin2 or a tetracycline Some pneumococci and Haemophilus influenzae strains tetracycline-resistant; approx. Suggested duration of treatment 5 days; longer treatment may be necessary in severely ill patients Suggested duration of treatment 5 days; longer treatment may be necessary in severely ill patients Alternative, clarithromycin5 1. Suggested duration of treatment 7 days (1421 days for infections caused by staphylococci) Pneumonia: high-severity community-acquired Benzylpenicillin + clarithromycin2 or benzylpenicillin + doxycycline If meticillin-resistant Staphylococcus aureus suspected, add vancomycin3. Suggested duration of treatment 710 days (may extend treatment to 1421 days in some cases. Suggested duration of treatment 14 days (usually 710 days for Legionella) Alternative if Legionella infection suspected, a quinolone If high-severity Legionella infection, add clarithromycin2 or rifampicin for the first few days. Suggested duration of treatment usually 710 days Suggested duration of treatment 14 days Alternative for chlamydial or mycoplasma infections, doxycycline Pneumonia: hospital-acquired Early-onset infection (less than 5 days after admission to hospital), co-amoxiclav or cefuroxime If life-threatening infection, or if history of antibacterial treatment in the last 3 months, or if resistant microorganisms suspected, treat as for late-onset hospital-acquired pneumonia. Suggested duration of treatment 7 days Late-onset infection (more than 5 days after admission to hospital), an antipseudomonal penicillin. For severe illness caused by Pseudomonas aeruginosa, consider adding an aminoglycoside. Suggested duration of treatment 7 days (longer if Pseudomonas aeruginosa confirmed) 1. Where amoxicillin is suggested ampicillin may be used Where clarithromycin is suggested azithromycin or erythromycin may be used Where vancomycin is suggested teicoplanin may be used Where cefotaxime is suggested ceftriaxone may be used 346.
Syndromes
- Acute ear infection
- Wearing a cast of brace to help with containment
- Loss of, or change in, sensation
- Testicular biopsy
- Blood studies (such as CBC, blood differential)
- Confusion
- Small painless sore on the male genitals or in the female genital tract
- You will usually be asked not to drink or eat anything for 6 to 12 hours before the procedure.
- Reduced movement on the side of the body with the dislocation
- Bleeding
Related Products
Usage: p.c.
Additional information:
8 of 10
Votes: 211 votes
Total customer reviews: 211
Customer Reviews
Deckard, 55 years: Hyperglycaemia and sometimes diabetes can occur with antipsychotic drugs, particularly clozapine, olanzapine, quetiapine, and risperidone. Foscavir (Clinigen) A Intravenous infusion, foscarnet sodium hexahydrate 24 mg/mL, net price 250-mL bottle = £119. This may therefore be a contraceptive method of choice for women who have excessively heavy menses.
Ford, 47 years: Indeed, evernimicin and avilamycin protect from chemical modification A2482 in H89 and A2534 in H91 [66, 67], while mutations in helices 89 and 91 confer resistance to evernimicin and a G2535A substitution causes avilamycin resistance [67, 68]. Bottom right: the possible interactions between L4 and L22 in its swung orientation [36]. Many pharmaceutical companies possess chemical libraries of protein kinase inhibitors that could be readily screened for infectious disease therapy.
Contact
0673406227
dppsmyanmar@gmail.com