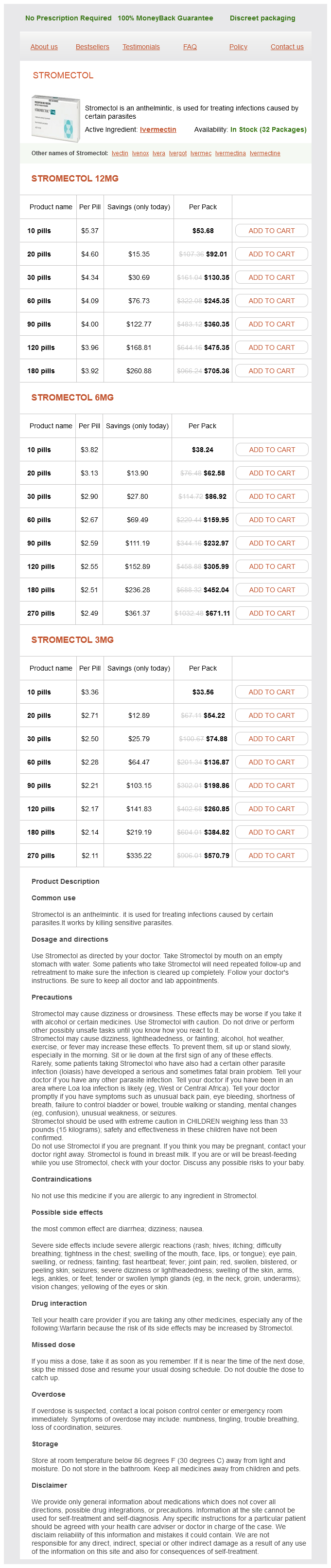
Stromectol
Stromectol 12mg
- 10 pills - $53.68
- 20 pills - $92.01
- 30 pills - $130.35
- 60 pills - $245.35
- 90 pills - $360.35
- 120 pills - $475.35
- 180 pills - $705.36
Stromectol 6mg
- 10 pills - $38.24
- 20 pills - $62.58
- 30 pills - $86.92
- 60 pills - $159.95
- 90 pills - $232.97
- 120 pills - $305.99
- 180 pills - $452.04
- 270 pills - $671.11
Stromectol 3mg
- 10 pills - $33.56
- 20 pills - $54.22
- 30 pills - $74.88
- 60 pills - $136.87
- 90 pills - $198.86
- 120 pills - $260.85
- 180 pills - $384.82
- 270 pills - $570.79
Stromectol dosages: 12 mg, 6 mg, 3 mg
Stromectol packs: 10 pills, 20 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills
In stock: 586
Only $2.25 per item
Description
There may be a familial or genetic contribution to keloid development as an autosomal dominant inheritance with incomplete penetrance antibiotic x-206 purchase 3 mg stromectol amex. For example, the ancient Olmec of Mexico in preColumbian times are one ethnic group which has used keloid scarification as an intentional means of decoration. Unlike scars, keloids are made up of markedly thickened bundles of collagen that are arranged in a haphazard fashion. Normal scar tissue formation, in contrast, consists of fibrillary bundles of collagen that are aligned parallel to the skin surface. It has been suggested that keloid fibroblasts fail to undergo physiologically programmed cell death and thereby produce extra connective tissue. Genetic factors are likely involved, and studies have identified four susceptibility loci. Keloids represent the end stage of an inflammatory process that starts after a traumatic disruption of skin integrity. Over a period of weeks, abnormally functioning fibroblasts replace the granulation tissue associated with the early stages of healing. Darkskinned individuals such as those of Asian, African, and Hispanic descent have a 15-fold increased risk to develop keloids compared to light-skinned individuals. Keloids are more commonly found on the ears, upper back and chest, and upper arms. Ongoing tension or movement across the wound healing site may predispose to keloid formation. Genetics are a factor, as there are reports of familial cases with varied modes of inheritance, indicating multiple genetic disorders that may influence keloid formation. Patients with specific rare inherited conditions like Goeminne syndrome and Rubinstein-Taybi syndrome are at increased risk of keloid formation. Age affects propensity to make a keloid with the highest incidence in individuals age 10 to 20 years. Dermatofibrosarcoma protruberans is an uncommon, locally aggressive cutaneous soft tissue sarcoma that may present as a plaque-like area of cutaneous thickening that may be violet-red or blue at the margins. The best treatment is prevention of unnecessary trauma or surgery, including ear piercing and elective cosmetic surgery. Early treatment of acne helps decrease inflamed pustules and papule formation, which, when located at the posterior neck, may become acne keloidalis nuchae. Patients with acne keloidalis nuchae should avoid shaving the neck region and instead should use scissors to trim hair no shorter than one-eighth of an inch. Consider varicella vaccination (Varivax)1 to decrease keloid risk of chickenpox lesions.
Sour Sop (Graviola). Stromectol.
- Use as an antibiotic, sedative, antiparasitic, cathartic, emetic; and for coughs, inflammation of the nose and throat, herpes, leishmaniasis (an infection caused by sand flies), cancer, and other conditions.
- How does Graviola work?
- Dosing considerations for Graviola.
- What is Graviola?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97005
In many patients antibiotic resistance how does it occur generic 6 mg stromectol mastercard, prednisone may be decreased to 5 mg every day or completely discontinued after 6 months. For patients who require a high dose of steroid for either clearing or maintenance, adjuvant therapy with another agent should be considered in order to avoid the long-term adverse effects of corticosteroids. These drugs include azathioprine1 (13 mg/kg/day in two equally divided doses), mycophenolate mofetil1 (1000 3000 mg/day or 40 mg/kg/day in two divided doses), and 1 950 methotrexate1 (1015 mg/week). The dose of the second drug may be decreased a few months after clinical remission, slowly tapered, and ultimately discontinued. Dapsone may be commenced at 25 to 50 mg/day and increased as needed by 25 mg every week until a beneficial effect is obtained. Antibiotics of the tetracycline family as well as erythromycin1 have been used alone or in combination with niacinamide1 and have been shown to have some benefit. The dose of tetracycline1 is 500 mg four times daily and niacinamide 500 mg three times daily. Minocycline1 or doxycycline1 in a dose of 100 mg twice daily may be substituted for patients who do not tolerate tetracycline. In patients with extensive disease, the addition of this combination to prednisone can have a corticosteroid-sparing effect. Therapy for mucous membrane pemphigoid varies with the disease location, extent, and severity. In limited oral disease, local therapy with topical anesthetic agents and topical glucocorticoids in addition to oral hygiene can suffice. The steroid may be applied under occlusion with a prosthetic device or may be injected intralesionally. In patients with severe oral disease and in patients with ocular, pharyngeal, or laryngeal involvement, systemic glucocorticoids, in combination with cyclophosphamide1 are indicated. In my experience, most patients have an excellent response, with a prolonged remission after treatment with the combination of prednisone (1 mg/kg/day for 6 months) and cyclophosphamide (12 mg/kg/day for 1824 months). Azathioprine1 and mycophenolate mofetil1 are generally less effective but may be used if there are contraindications to steroid or cyclophosphamide use. Patients with severe ocular scarring might benefit from cryotherapy ablation of eyelashes. Epidermolysis Bullosa Acquisita Unlike bullous pemphigoid and other subepidermal autoimmune bullous diseases, epidermolysis bullosa acquisita is generally resistant to therapy. Trauma contributes to blister formation, especially in the classic form of epidermolysis bullosa acquisita. The inflammatory form of epidermolysis bullosa acquisita responds more easily to therapy than the classic form. Because of the neutrophil predominance in the inflammatory form, patients might respond to dapsone.
Specifications/Details
Adequately controlled hypertension should not confer any additional risk for altitude illness antibiotic resistance action center 3 mg stromectol purchase free shipping. Any patient requiring more than one medication or maximum dose of one medication should travel with a blood pressure cuff and monitor their blood pressure. These patients should also develop an algorithm with their physician for how to manage elevated blood pressure and when to decrease or hold doses. All patients with known history or antecedent symptoms should undergo risk stratification, cardiac stress testing, and consult with their cardiologist. It is advisable to avoid exertion until acclimatized, or for at least 4 to 5 days. Subsequent exertion should be below tolerated exertion at their elevation of residence, and strenuous exercise should be avoided. Other patients, including those with abnormal stress tests, angina, or acute coronary syndrome within six months without revascularization, should not travel to altitude. Diabetes Mellitus Heart Failure High altitude may increase risk for decompensation of chronic heart failure, and patients with poorly compensated heart failure should avoid travel. If heart failure is stable and controlled, patients may tolerate travel to altitude less than 3000 meters, but physical activity should remain below what is tolerated at their altitude of residence. These patients should monitor their body weight and develop an algorithm with their physician for how to adjust diuretics for increasing edema or weight gain. Allergic asthma will likely improve at high altitude, but asthma that is exercise- or cold-induced may be made worse. An optimized pre-travel medical regimen should be continued, and these patients should travel with additional rescue medications, including bronchodilators and corticosteroids. Patients should travel with an up-to-date asthma action plan and know where to seek medical attention for an exacerbation that cannot be managed independently. Travel should be avoided in moderate persistent or severe asthma, history of hospitalization, or recent exacerbation. Those who are chronically hypoxemic may have some tolerance to hypobaric hypoxia due to their adaptations to chronic hypoxia. Data is more limited on patients with chronic carbon dioxide retention, and these patients should avoid travel to high altitude. The elevated risk for cerebrovascular accident in diabetics may be further increased at high altitude. Basal metabolic rate will increase, appetite may be suppressed, and absorption may be slowed, but hypoxia also causes hyperglycemia. Glucose-monitoring devices may lose accuracy, though glucose dehydrogenase-based glucometers may have more reliable performance. Hydration is also particularly important for diabetic patients, particularly type 1, which can be self monitored by urine output and color. Despite the above changes at altitude that suggest later administration of prandial insulin, there may also be a delay in the effects of rapid-acting insulin with increasing elevation, which may require earlier administration. This will also be affected by rate of ascent, acclimatization, exertion, and of course diet.
Syndromes
- Nausea?
- Complete blood count (CBC)
- Overextend the knee joint
- Medicines taken by mouth or through an IV to help remove fluid from the body
- Very strong hydrocortisone creams (available by prescription) are recommended for badly chapped hands
- Crusting
Related Products
Usage: p.r.n.
Additional information:
9 of 10
Votes: 121 votes
Total customer reviews: 121
Customer Reviews
Ivan, 28 years: Epinephrine and dopamine should not be used because -receptor stimulation in the presence of -receptor blockade may provoke dysrhythmias and phenothiazines are antidopaminergic. Hormone receptorpositive breast cancer, meaning progesterone or estrogen receptorpositive, is the most common type of breast cancer, comprising more than 65% of all breast cancers and in general has less aggressive disease course with a long survival, even in the metastatic setting.
Mazin, 57 years: All stuporous and comatose patients should have glucose (for hypoglycemia), thiamine (if chronically alcoholic), and naloxone (Narcan) (in case of an opioid ingestion) intravenously and should be admitted to the intensive care unit. Hybrid closedloop technology can be particularly useful for overnight glycemic control, when many patients and families are most fearful of hypoglycemia.
Peratur, 36 years: Age may be a risk factor in the development of bullous pemphigoid and mucous membrane pemphigoid. Chemical Burns the risk and degree of injury caused by chemical burns vary greatly, depending on the substance involved as well as on the concentration of the material and the duration of exposure.
Grimboll, 34 years: Children who have had an apparent severe allergic reaction to a vaccine should be evaluated by an allergist to determine the responsible allergen and to make recommendations regarding future vaccination. On physical examination, the patient may have fever, decreased bowel sounds, diffuse lower abdominal tenderness with rebound tenderness, and/or right upper quadrant tenderness.
Keldron, 26 years: Viperid snake envenomation invariably results in tissue injury, manifested by pain and progressive swelling, and it may include ecchymosis, elevated tissue and compartment pressures, tissue necrosis, and tissue loss. Presence/absence of sleepiness, fatigue, and irritability/hyperactivity are all important.
Contact
0673406227
dppsmyanmar@gmail.com