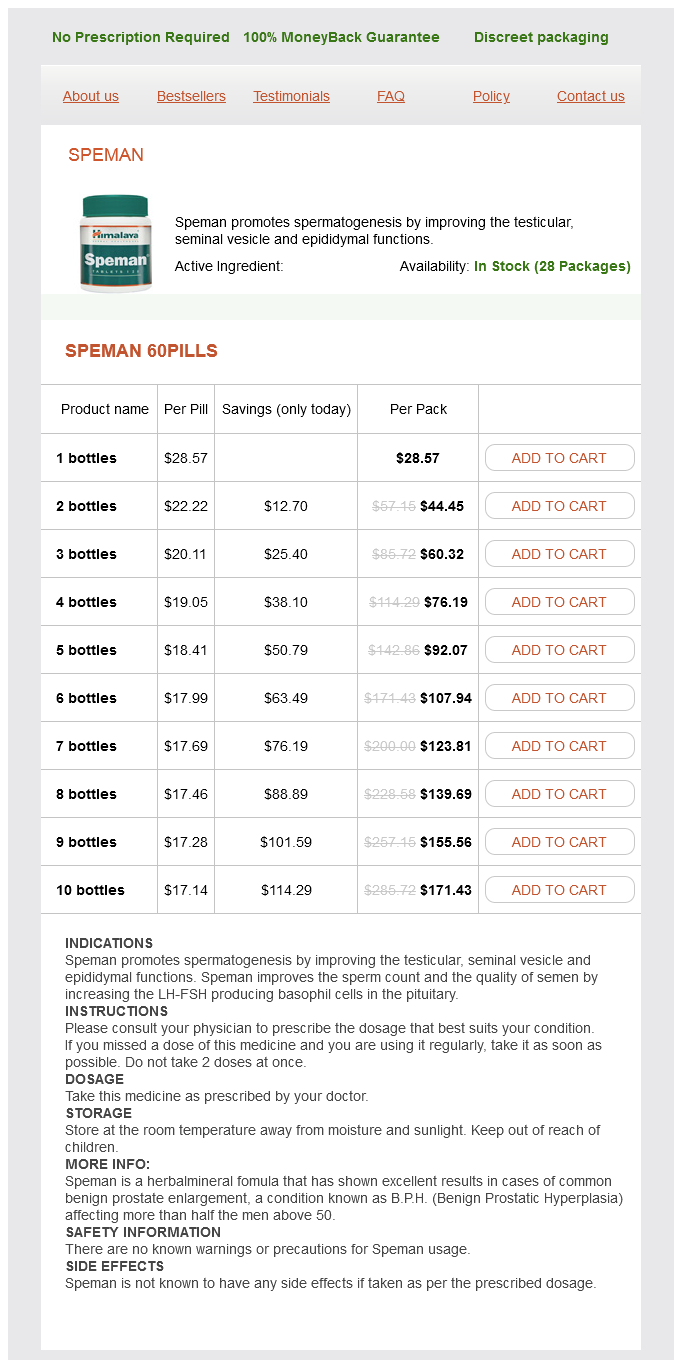
Speman
Speman 60pills
- 1 bottles - $28.57
- 2 bottles - $44.45
- 3 bottles - $60.32
- 4 bottles - $76.19
- 5 bottles - $92.07
- 6 bottles - $107.94
- 7 bottles - $123.81
- 8 bottles - $139.69
- 9 bottles - $155.56
- 10 bottles - $171.43
Speman dosages: 60 pills
Speman packs: 1 bottles, 2 bottles, 3 bottles, 4 bottles, 5 bottles, 6 bottles, 7 bottles, 8 bottles, 9 bottles, 10 bottles
In stock: 780
Only $18.21 per item
Description
The bleeding is a slightly brownish colour and continuous prostate oncology times buy discount speman 60 pills online, and clots are rarely present (Table 12. Two clinical patterns occur and are due to the extent of the dam age to the tubal wall by the invading trophoblast. Occasionally there is an attack of sharp pain and faintness, owing to an episode of intraperitoneal bleeding, and if these sym ptom s are m arked, and particularly if the episode is followed by slight vaginal bleeding, exam ination m ay reveal tenderness in the lower abdom en; vaginal exam ination m ay show a tender fornix or a vague m ass, but the signs m ay be insuf cient to m ake a diagnosis. Further episodes of pain are likely and the blood loss per vaginam persists until acute collapse supervenes (indicating tubal rupture or incom plete tubal abortion) or the sym ptom s cease (indicating com plete abortion with or without a pelvic haem atocele). It is m ore usual for the acute rupture to supervene upon the subacute, but the m ild sym ptom s of the latter m ay have been thought to be norm al occurrences in pregnancy and ignored. As the tube ruptures the patient is seized with a sudden acute lower abdom inal pain, suf ciently severe to cause fainting. The associated internal haem orrhage leads to collapse, pallor, a weak, rapid pulse and a falling blood pressure. Usually the condition im proves after a short tim e as the haem orrhage dim inishes or ceases, but abdom inal discom fort persists, and pain is felt in the epigastrium or is referred to the shoulder. A further episode of haem orrhage and collapse is likely, and continued bleeding can be suspected from increasing pallor and a falling haem oglobin level. On exam ination the patient is in shock and the lower abdom en is tender, with som e fullness and m uscle 116 Chapter 1 2 Extra-uterine pregnancy/ectopic gestation guarding. Vaginal exam ination, which should only be carried out in hospital, shows extrem e tenderness on m ovem ent of the cervix from side to side. If she is in shock, an intravenous line should be set up and transfer quickly arranged. As m entioned, if there is any doubt about the diagnosis a pelvic ultrasound exam ination should be carried out to establish whether the pregnancy is intra- or extra-uterine. Once the ectopic gestation has been diagnosed, the treatm ent is usually surgical or in selected cases m edical. The gynaecologist m ay: · Insert a laparoscope to inspect the Fallopian tube and, if possible, under laparoscopic vision incise along the superior border and suck the ectopic gestation out of the tube. Laboratory tests m ay help, but in m ost instances they are not particularly inform ative. The levels should double every 48 hours, a rise <66% being suggestive of an ectopic gestation. On the other hand, if ultrasound shows an intra-uterine pregnancy, a concurrent ectopic pregnancy is extrem ely unlikely. Routine serum progesterone levels can help to exclude an ectopic pregnancy (>79 nm ol/L) and identify a nonviable pregnancy (>15. If ultrasound is not available, or the result is equivocal, the presum ptive diagnosis should be con rm ed by laparoscopy.
Rhizoma Pinelliae (Pinellia Ternata). Speman.
- Dosing considerations for Pinellia Ternata.
- How does Pinellia Ternata work?
- Are there safety concerns?
- Nausea, morning sickness, cough, birth control, influenza (flu), and inflammation.
- What is Pinellia Ternata?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97039
In childhood the labia m ajora contain little adipose tissue prostate ultrasound speman 60 pills lowest price, and in older age the adipose tissue disappears. The labia m inora are at, delicate folds of skin containing connective tissue and som e sebaceous glands, but no adipose tissue. On their m edial aspect the keratinized epithelium of the skin changes into poorly keratinized squam ous epithelium, containing m any sebaceous glands. Anteriorly, the labia m inora split into two parts, one passing over the clitoris to form the prepuce of the organ, the other passing beneath to form the hom ologue of the frenulum of the m ale. Posteriorly, they fuse to form the fourchette, which is always torn during parturition. In the reproductive years the labia m inora are hidden by the labia m ajora, but in childhood and old age they appear to be m ore prom inent as the labia m ajora are relatively sm all. The size of the labia m inora varies considerably in different wom en, but this is of little clinical im portance. The proxim al two-thirds of the internal surface of the labia m inora and all the tissues internal to them are derived from the endoderm. The distal third of the internal surface of the labia m inora and all of the vulva external to this is derived from the ectoderm, and the histology is that of the skin. The cleft between the labia m inora is called the vestibule, and contains the external urethral m eatus and the hym en, which lies just inside and surrounds the vaginal ori ce. They form the lateral boundaries of the vulval cleft and are the hom ologues of the scrotum. Mons Labium majus External urethral orifice Labium minus Vaginal orifice Posterior commissure Prepuce Glans Frenulum of Clitoris V estibule Hymen Fourchette is the hom ologue of the penis, and is com posed of erectile tissue. Only the glans and prepuce of the clitoris are norm ally visible, but the corpus can be palpated along the lower surface of the sym physis pubis as a cord-like structure. The hym en is a thin, incom plete m em brane surrounding the vaginal ori ce, and has one or m ore apertures in it that allow m enstrual blood to escape. The apertures are of various shapes and sizes and the hym en varies considerably in elasticity, but is generally torn during a rst coitus. In attem pting to m ake a decision regarding virginity, palpation to feel a circular ridge of hym enal tissue is m ore accurate than inspection. Although the hym en is relatively avascular, tearing at rst coitus m ay be accom panied by a sm all am ount of bleeding, which ceases rapidly. Just lateral to the hym en, surrounding the vaginal ori ce on each side and deep to the bulbocavernosus m uscle (the sphincter vaginae), are two collections of erectile tissue the vestibular bulbs. It is connected to the posterior part of the vestibule, between the hym en and the fourchette, by a duct som e 2 cm in length. Ve ins the veins of the vulva form large venous plexuses, which becom e dilated during sexual excitem ent, and to an even greater degree during pregnancy, when varicosities are not uncom m on.
Specifications/Details
Listen for: · pleural rub; · heart murmur associated with acute tricuspid regurgitation; · additional heart sounds (gallop rhythm) prostate cancer jewelry generic 60 pills speman, widely split second heart sound. Pulmonary embolus In severe cases · Secure venous access (16 G cannula or larger); give a fluid challenge, 500 mL of warmed crystalloid or colloid. This should be repeated up to a volume of 2 L if a satisfactory response is not obtained. Hypotension this is a common reason for being called to see an acutely unwell patient, particularly in the postopera tive period. After elimination of airway and breathing problems as a cause for the hypoten sion, examine the patient for the following signs and symptoms. Investigations · Chest Xray: often unremarkable although occasionally one or both pulmonary arteries appear prominent and a peripheral wedgeshaped abnormality in one of the lung fields may be secondary to pulmonary infarction. Specific features suggesting right heart strain and the classic S1, Q3, T3 pattern are rarely seen, and have a low negative predictive value when absent. Look for: · evidence of impaired cerebral perfusion; conscious level: orientated good; confused/agitated bad; unresponsive worse; · tachypnoea, dyspnoea; · colour: pale, cyanosed, flushed; Perioperative medical emergencies: recognition and management 153 · sweating; · neck veins: collapsed or distended (raised jugular venous pressure). Listen for: · abnormal breath sounds; fine inspiratory crackles and/or (cardiac) wheeze; · the presence of additional heart sounds (gallop rhythm) or a murmur; · altered or absent breath sounds. In the postsurgery patient, ongoing haemorrhage will be suggested by: · a large volume of blood in the surgical drains, or from a wound; · a distending abdomen; · wound swelling. Feel for: · pulse: rate, volume (central for example carotid, femoral and peripheral, for example radial, dorsalis pedis) and regularity; · capillary refill time: firm pressure applied over the sternum (central refill time) and to a digit (peripheral refill time) for 5 seconds to produce blanching; prompt return of colour within 2 seconds maximum is normal; delayed peripheral capillary refill suggests a low cardiac output and/or perfusion pressure, delayed central capillary refill is an ominous sign; unreliable in hypothermic patients; · position of the apex beat; · position of the trachea. Because of its common usage, the following types of shock are covered in more detail below: · · · · hypovolaemic shock; septic shock; anaphylactic shock; cardiogenic shock. Start treatment · All patients should be given oxygen via a facemask and reservoir at a flow rate of 15 L/minute. The choice of fluid (crystalloid versus colloid) is not as important as the fact that some fluid is being given. Avoid dextrosecontaining fluids, as they rapidly distribute throughout the total body water and have minimal intravascular effect. In addition, they cause hyperglycaemia, which is associated with increased mortality in critically ill patients. Metabolic acidosis signified by low pH, high negative base excess and elevated Hypovolaemic shock Common causes of hypovolaemia include bleeding (external or concealed), excessive losses from the gas trointestinal tract (for example, diarrhoea, vomiting, fistula loss), excessive third space losses after major tissue trauma and the relative hypovolaemia that occurs with epidural anaesthesia. Specific findings in hypovolaemia are manifesta tions of the increase in sympathetic outflow: 154 Perioperative medical emergencies: recognition and management · · · · serum lactate is found proportionate to the severity and duration of the shock state. Even if the patient has a satisfactory response to the fluid challenge, help will often still be required for definitive treatment. Acute haemorrhage, which may be overt or covert, must be controlled and this may require the urgent transfer of the patient to the operating theatre or interventional radiology. The resuscitation fluid in these circumstances is blood; however, haemostasis has a higher priority than restoration of a normal blood pressure. Rapid, highvolume fluid resuscitation will exacerbate bleeding and is associated with a worse prognosis.
Syndromes
- Over 4 months old -- if the baby has begun solid foods, try baby foods with high-fiber content (peas, beans, apricots, prunes, peaches, pears, plums, spinach) twice a day.
- Any symptoms of this disorder
- Is often relieved by sitting up and leaning or bending forward
- Factor V Leiden
- Weakness
- Weight gain
- The health care provider holds your head in a certain position and asks you to lie quickly backward over a table.
Related Products
Usage: p.c.
Additional information:
10 of 10
Votes: 97 votes
Total customer reviews: 97
Customer Reviews
Phil, 23 years: The authors found that 10 mg of intramuscular morphine was more efficacious than 60 mg of intramuscular codeine in terms of pain relief.
Mojok, 53 years: With arms kept at the sides, the patient is turned in two stages firstly into the lateral position and then prone.
Randall, 55 years: A feeding bottle should be avoided as it m ay stop the baby from learning how to suck properly at the breast.
Alima, 30 years: The reflex response is an increase in sympathetic discharge causing tachycardia, increase in stroke volume and cardiac output.
Sebastian, 58 years: In some patients these two layers can be distin guished separately, particularly at the dorsum where the deep dorsal vein runs between them, but in general the distinction is hard to make.
Barrack, 60 years: Giving sets and fluid warmers Fluid and blood are administered to the patient from a bag hung on a drip stand through a giving set connected to the LuerLok fitting on the intravenous cannula.
Tangach, 46 years: Intravenous fluids are often at ambient tempera ture (20 °C), while blood and blood products may be as cold as 4 °C when given, which can lead to significant cooling of the patient; to prevent this, flu ids are often warmed as they are being given.
Kapotth, 48 years: As piped gases are already deliv ered at 400 kPa, no further pressure reduction is required.
Contact
0673406227
dppsmyanmar@gmail.com