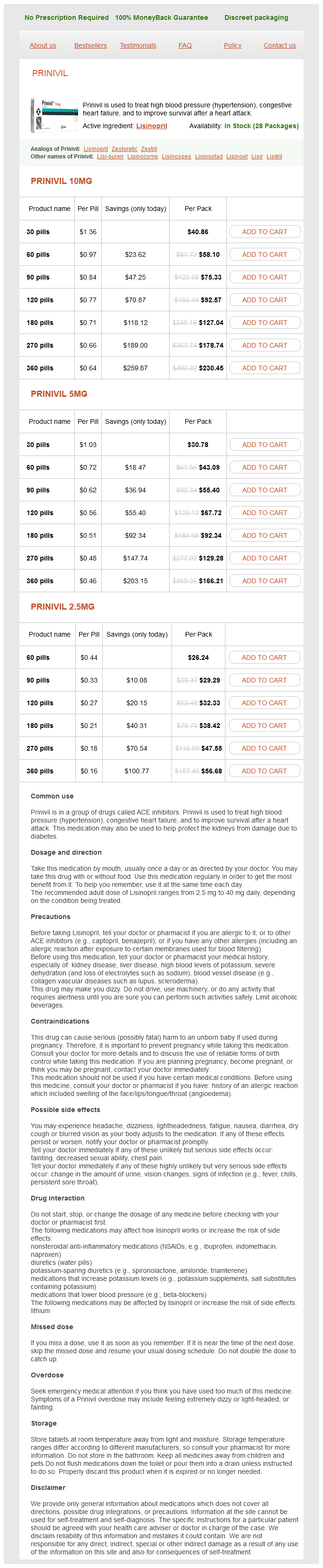
Prinivil
Prinivil 10mg
- 30 pills - $40.86
- 60 pills - $58.10
- 90 pills - $75.33
- 120 pills - $92.57
- 180 pills - $127.04
- 270 pills - $178.74
- 360 pills - $230.45
Prinivil 5mg
- 30 pills - $30.78
- 60 pills - $43.09
- 90 pills - $55.40
- 120 pills - $67.72
- 180 pills - $92.34
- 270 pills - $129.28
- 360 pills - $166.21
Prinivil 2.5mg
- 60 pills - $26.24
- 90 pills - $29.29
- 120 pills - $32.33
- 180 pills - $38.42
- 270 pills - $47.55
- 360 pills - $56.68
Prinivil dosages: 10 mg, 5 mg, 2.5 mg
Prinivil packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 512
Only $0.17 per item
Description
Treatment Chronic subdural hematomas are treated with surgical drainage unless they are small and asymptomatic blood pressure after exercise discount prinivil 10 mg buy line. Alternative Diagnosis: Idiopathic Intracranial Hypertension Textbook Presentation Patients tend to be young women who are obese. Headaches caused by idiopathic intracranial hypertension are severe, occur daily, and may awaken the patient from sleep. Idiopathic intracranial hypertension is frequently referred to as pseudotumor cerebri. The characteristics of idiopathic intracranial hypertension were well described from a series of patients in the early 1990s. Visual disturbances (usually lasting only seconds) and pulsatile tinnitus are also common. The presence of papilledema is a very important finding in idiopathic intracranial hypertension. Idiopathic intracranial hypertension carries the risk of permanent visual loss and must be diagnosed and treated. The diagnosis of idiopathic intracranial hypertension is based on recognition of the headache syndrome, diagnosis of increased intracranial pressure, and exclusion of other causes of increased pressure. The headache in idiopathic intracranial hypertension must occur daily, be diffuse and/or constant, or be aggravated by coughing. Generally first detected on a physical exam by the presence of papilledema, an enlarged blind spot, a visual field defect, or a sixth cranial nerve palsy. To make the diagnosed, intracranial hypertension must be demonstrated on lumbar puncture (> 200 mm H2O in nonobese patients, > 250 mm H2O in obese patients). The headache must improve after lumbar puncture (with a postprocedure pressure of 120170 mm H2O) and resolve after treatment of idiopathic intracranial hypertension. Over the next 2 years, multiple attempts at weaning corticosteroids failed, and the patient continues to take 15 mg of prednisone. While taking prednisone, a spinal compression fracture, acne, diabetes mellitus, and difficult-to-control hypertension develop. This is probably not high enough to accept the side effects of long-term prednisone therapy without a more definitive diagnosis. The presentation of fever and headache is common and can be worrisome, potentially caused by anything from influenza to meningitis. Although certainly not the most common cause of fever and headache, meningitis is a relatively common, potentially life-threatening illness. Viral causes are 34 times more common than bacterial causes and have a generally favorable prognosis. Mortality rates vary by organism but community-acquired bacterial meningitis has a mortality rate of about 25%. A review studied patients in Holland in whom community-acquired bacterial meningitis was diagnosed over a 3 1/2 year time period; the prevalence of various exam features follow: 1.
Arusa (Malabar Nut). Prinivil.
- How does Malabar Nut work?
- Are there safety concerns?
- What is Malabar Nut?
- Dosing considerations for Malabar Nut.
- Coughs, breathing problems, spasms, and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96051
Gastrografin is hyperosmolar and draws fluid into bowel lumen prehypertension systolic normal diastolic buy 10 mg prinivil mastercard, potentially dilating bowel. Careful, frequent observation and repeated physical exam over the first 1224 hours C. Broad-spectrum antibiotics (59% of patients have bacterial translocation to mesenteric lymph nodes) E. Signs of ischemia (increased pain, fever, tenderness, peritoneal findings, acidosis, or worsening leukocytosis) 2. Some clinicians recommend surgery when bowel obstruction fails to resolve in 24 hours. Alternative Diagnosis: Ischemic Bowel Secondary to Acute Mesenteric Ischemia or Ischemic Colitis Ischemic Bowel Three distinct clinical subtypes of ischemic bowel include chronic mesenteric ischemia (chronic small bowel ischemia), acute mesenteric ischemia (acute ischemia of small bowel), ischemic colitis (ischemia of the large bowel). Acute Mesenteric Ischemia Textbook Presentation Acute mesenteric ischemia is a life-threatening condition that virtually always presents with the abrupt onset of acute severe abdominal pain that is typically out of proportion to a relatively benign physical exam. Acute mesenteric ischemia usually occurs in patients with risk factors for systemic embolization (eg, atrial fibrillation) or arterial thrombosis. Etiology: Usually due to superior mesenteric artery or celiac artery embolism (50%). Other causes include thrombosis (1525%), low flow states without obstruction (1530%) (nonobstructive mesenteric ischemia), and mesenteric venous thrombosis (5%). Risk factors include atrial fibrillation, acute myocardial infarction, valvular heart disease, heart failure, ventricular aneurysms, angiography of abdominal aorta, and hypercoagulable states. Approximately half of such patients have a prior history of chronic mesenteric ischemia with intestinal angina. Often occurs in elderly patients with mesenteric atherosclerotic disease and superimposed hypotension (due to myocardial infarction, heart failure, dialysis, or sepsis). Alpha-agonists, digoxin, and betablockers may also increase the risk of nonobstructive mesenteric ischemia. Also seen in critically ill patients after cardiopulmonary bypass or other major surgery d. Other causes include cocaine use and following endurance exercise activities (eg, marathon, cycling). Mesenteric venous thrombosis is often secondary to portal hypertension, hypercoagulable states, and intra-abdominal inflammation. Patients have acute abdominal pain that is often out of proportion to their abdominal exam. Common presenting symptoms are abdominal pain (94%), nausea (56%), vomiting (38%), and diarrhea (31%). Plain abdominal radiographs may reveal thickening of bowel loops or thumbprinting but are insensitive (40%). One study reported 100% sensitivity but patients were studied 3 days after symptom onset, when infarction may have been easier to demonstrate.
Specifications/Details
Dissection of the upper pouch should be sufficient to allow an opening to be made in the distal end for an anastomosis to be performed heart attack one direction song discount 10 mg prinivil with visa. As with the lower esophagus, branches of the vagus supplying the upper esophagus should not be disturbed. A stay suture can be placed in the muscular wall of the esophagus to facilitate its exposure and minimize the need for forceps traction. The size of the opening in the upper esophagus should correspond to the diameter of the lower esophagus. Unless the two ends of the esophagus are very close together, all the sutures are placed in position in the posterior layer before they are tied in sequence. The sutures with the attached forceps are crossed over and gradual tension applied, bringing the proximal and distal halves of the posterior esophagus toward each other. The use of a nerve hook avoids the need to use forceps on the open ends of the esophagus when placing the sutures. The surgeon stands on the left side of the table with the screen opposite at the right upper end of the table. Assistant Surgeon 15 operation 137 Insertion of cannula 16 Three cannulae are inserted in the right chest in a V-shape. Occasionally, if the lung does not collapse completely, it may be necessary to introduce a further 3-mm port posterior to the other two working ports to retract the lung anteriorly using an atraumatic forceps. The mediastinal pleura covering the proximal esophageal blind pouch is opened and the pouch mobilized. For guidance, the anesthetist pushes on the Replogle tube in the proximal esophagus. The fistula is now transected and air leak from the trachea is excluded by Valsalva maneuver. To mobilize the upper pouch, it is useful to insert a traction suture of Vicryl 4/0 in the pouch and dissect it from the trachea. By leaving the end of a suture a little longer, traction can be applied so that the next suture can be placed more easily. Regular chest physiotherapy, with nasopharyngeal suction, as required, is carried out to avoid respiratory infection. To avoid a prolonged intraoperative acidosis and hypercapnia, consideration should be given to (1) reducing the insufflation pressure or totally avoiding insufflation; (2) pausing the operation and allowing the acidosis to correct; or (3) converting the operation to the open procedure. A retrospective study of 104 infants reported that 12 percent of infants developed an early leak or stricture at the anastomosis and 32 percent required at least one esophageal dilatation. Consideration should be given to re-exploration of the anastomosis with the intention of repairing the leak. Risk factors include anastomotic tension, anastomotic leakage, and gastroesophageal reflux. The esophagostomy may be sited on either side of the neck, but the left side is preferred, as it is more suited to the anastomotic site following esophageal replacement. A transverse incision is made on the left side of the neck 1 cm above and parallel to the medial third of the clavicle.
Syndromes
- Memory disorders
- The surgeon may use real bone or fat tissue, or an implant made out of silicone, Teflon™, Dacron, or newer biological inserts.
- Collapse
- Permanent changes in skin color
- Central nervous system disorders (neurosyphilis)
- Dry cough
Related Products
Usage: p.r.n.
Additional information:
10 of 10
Votes: 43 votes
Total customer reviews: 43
Customer Reviews
Tom, 61 years: A second layer of non-absorbable sutures including the seromuscular surface of the stomach only may be placed superficial to the primary sutures to prevent disruption of the wrap.
Altus, 64 years: Monitoring following dilatation should be carried out in a designated recovery area immediately following dilatation and should include regular measurements of pulse, heart rate, temperature, and blood pressure.
Gonzales, 65 years: Listening closely to patients with migraines describe their aura will make it easy to recognize auras in other patients.
Wenzel, 37 years: Proteinuria (> 5001000 mg/day), elevated serum creatinine, or hypertension suggests more severe or progressive disease and are indications for renal biopsy to establish the diagnosis.
Chenor, 54 years: Although there was no clinically significant rebleeding, other complications developed.
Bernado, 58 years: For all patients with viral pneumonias, a high clinical suspicion of bacterial superinfection should be maintained.
Falk, 23 years: Bladder dysfunction (1) Initially motor function normal, but sensation of bladder distention impaired (2) Then, detrusor muscle hypocontractility occurs, leading to urinary retention and overflow incontinence.
Contact
0673406227
dppsmyanmar@gmail.com