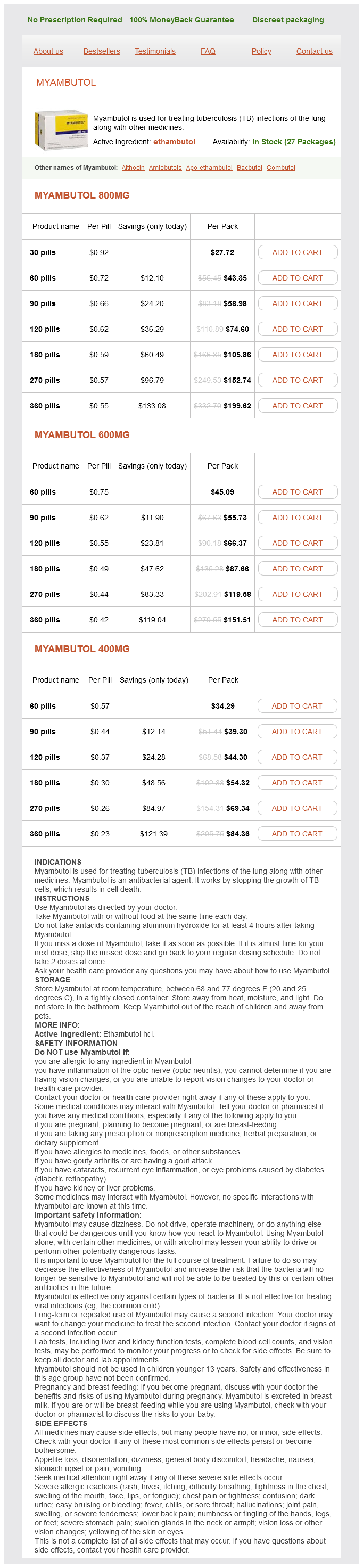
Myambutol
Myambutol 800mg
- 30 pills - $27.72
- 60 pills - $43.35
- 90 pills - $58.98
- 120 pills - $74.60
- 180 pills - $105.86
- 270 pills - $152.74
- 360 pills - $199.62
Myambutol 600mg
- 60 pills - $45.09
- 90 pills - $55.73
- 120 pills - $66.37
- 180 pills - $87.66
- 270 pills - $119.58
- 360 pills - $151.51
Myambutol 400mg
- 60 pills - $34.29
- 90 pills - $39.30
- 120 pills - $44.30
- 180 pills - $54.32
- 270 pills - $69.34
- 360 pills - $84.36
Myambutol dosages: 800 mg, 600 mg, 400 mg
Myambutol packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 643
Only $0.25 per item
Description
Imaging of peripheral nerve sheath tumors with pathologic correlation: pictorial review infection knee joint safe myambutol 800 mg. International consensus statement on malignant peripheral nerve sheath tumors in neurofibromatosis. Tumors of the peripheral nervous system: analysis of prognostic factors in a series with long-term follow-up and review of the literature. Hence, if the impact has not killed the patient, there is opportunity to intervene and minimize further morbidity or mortality. On-scene diagnostics may enable brain injury-specific therapies to be targeted in future. It is, however, the role of scientists and clinicians to minimize the effects of secondary brain injury, be that through the development of techniques and drugs to reduce evolving injury or through the development of systems to deliver specific treatments in a hyperacute manner. If you are not dead when the emergency services arrive, there is an interventional opportunity and you should not die-it is our ability to control secondary injury that determines this outcome. Mechanisms of Injury the most common causes of head injuries are road traffic incidents, falls, and assaults. Although contact sport injuries attract attention for concussion and return-to-play reasons, they are not usually immediately life threatening. The mechanism of injury and patient features can help to predict underlying brain injury. Direct blows to the head are more likely to result in skull fractures and extradural hematoma. This relates to the use of firearms in suicide (the most common suicide mechanism in males) and gang feuds. It is vital that hyperacute pathologic processes are appreci~ ated so that correct treatments can be developed. There is some evidence that rapid reoxygenation can worsen microhemor~ rhage formation,6 but this needs further study. Impact Brain Apnea Although commonly forgotten, one of the first responses fol~ lowing a blow to the head is a period of apnea. The volume of microhemorrhage appears to correlate with neuro~ logic outcome following abusive head trauma (nonaccidental injury/shaken baby syndrome). And despite the consid~ erable media attention this issue has received, many more people are "concussed" through domestic, occupational, and traffic accidents than sports. While approaching the patient, signs as to the mechanism and force vectors of injury can often be evaluated by "reading the wreckage.
Sardian Nut (European Chestnut). Myambutol.
- How does European Chestnut work?
- Are there any interactions with medications?
- Are there safety concerns?
- Dosing considerations for European Chestnut.
- Bronchitis, whooping cough, nausea, diarrhea, stomach problems, circulation problems, fever, infections, kidney disorders, muscle pain, sore throat, wounds, and other conditions.
- What is European Chestnut?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96522
VtsualWttion of peripheral nerve degeneration and regeneration: monitoring with diffiuion tensor tractography antibiotics rosacea order myambutol 400 mg on line. Ultrasound as a useful tool in the diagnosis and management of trawnatic nerve lesions. Peroneal nerve palsy associated with knee luxation: evaluation by sonography-initial experiences. Examination of postoperative peripheral nerve lesions with high-resolution sonography. Double fascicular nerve transfer to the biceps and brachialis muscles after brachial plexus injury: clinical outcomes inaserie. Nerve transfers to the biceps and brachialis branches to improve dhow flexion strength afi:er brachial plexus injuries. Experimental study on donor nerves for brachial plexus injury: comparison between the spinal accessory nerve and the intercostal nerve. Results of nerve transfer techniques for restoration of shoulder and elbow function in the context of a meta-analysis of the English literature. Evaluation of suprascapular nerve neurotization after nerve graft or transfer in the treatment of brachial plexus traction lesions. Nerve transfer to ddtoid muscle using the nerve to the long head of the triceps, part I: an anatomic feasibility study. Shoulder muscle reconstruction in the upper type of the brachial plexus injury by partial radial nerve transfer to the axillary nerve. Transfer of pectoral nerves to the musculocutaneous nerve in obstetric upper brachial plexus palsy. Evaluation of intercostal to musculocutaneous nerve transfer in reconstructivt: brachial plexus surgery. Restoration of elbow flexion in brachial plexus avulsion injury: comparing spinal accessory nerve transfer with intercostal nerve transfer. Brachial plexus neurotization with donor phrenic nerves and its effect on pulmonary function. Restoration of elbow flexion in brachial plexus injury by transfer of ulnar nerve fascicles to the nerve to the biceps muscle. Transfer of fascicles from the ulnar nerve to the nerve to the biceps in the treatment of upper brachial plexus palsy. A new method for treatment of facial palsy: the cross-face nerve transplantation with end-to-side neurorrhaphy. Alternativt: approach using the combined technique of nerve crossavt:r and cross-nerve grafting for reanimation of facial palsy. Functional upgrading of partially recovered facial palsy by cross-face nerve grafting with distal end-to-side neurorrhaphy.
Specifications/Details
Venical dislocation is due to the incompetence of the atlantoaxial joint and lateral masses antibiotic abuse buy myambutol 800 mg with mastercard. Mobile and Reducible Atlantoaxial Dislocation In 200 1 the author and colleagues analyzed 160 cases with mobile and reducible atlantoaxial dislocation treated in our department from 1988 to 2001. Clinical Features Pain and spasm in the upper part of the neck and restriction of neck movements are common symptoms. The patient may give a history of an injury that flexed the head and neck (such as when one is hit on the back of the head) as the precipitating factor. Severe injuries to the cervicomedullary cord may produce quadriparesis/ quadriplegia, respiratory paralysis, coma, and even death. It is not neural deformation but repeated microtraurna due to instability that is the prime cause of symptoms. Bone fusion takes about 3 months, and the metal implants should be strong enough to hold the region for that period and provide a zero movement environment. It ultimately depends on bone fusion to provide stability to the region and to hold the implant in position. Such information can be crucial when lateral mass fixation techniques are employed. Three-dimensional (3D) Cf scanning and 3D model reconstruction are emerging as useful imaging modalities. The operative subtleties and instrumentation can be identified, rehearsed, and practiced prior to surgery. The artery has multiple loops and an intimate relationship with the atlas and axis bones. The shape, size, and location of the vertebral artery groove on the inferior aspect of the superior articular facet of the C2 and over the posterior arch of the atlas have wide variations. Throughout its course, the vertebral artery is covered with a large plexus of veins. The venous plexuses are the largest in the region of the lateral gutter posterior to the Cl-C2 joint. After a relatively linear ascent of the vertebral artery in the foramen transversarium of C6 to C3, the artery makes a loop medially toward an anteriorly placed superior articular facet of the C2 vertebra, making a deep groove on its inferior surface. The presence of venous congestion provides support to the arterial movements, and veins dilate and empty on head turning and twisting. The superior facet of the C2 vertebra differs from the facets of all other vertebrae in two important characters. Second, the vertebral artery foramen is present partially or completely in the inferior aspect of the superior facet of C2, whereas in other cervical vertebrae, the vertebral artery foramen is located entirely in relationship with the transverse process. Unlike superior facets of all other vertebrae, they do not form a pillar with the inferior facets, being considerably anterior to them. The course of the vertebral artery in relationship to the inferior aspect of the superior articular facet of the C2 makes it susceptible to injury during transarticular and interarticular screw implantation techniques. The inferior facet of the atlas and superior facet of the axis are almost flat and Treatment the surgical management of craniovertebral anomalies is complex due to the relative difficulty of accessing the region, the critical relationships of neurovascular structures, and the intricate biomechanical issues involved.
Syndromes
- Urine and fecal urobilinogen
- Common cold
- Acromegaly
- Activated charcoal
- You are pregnant or could be pregnant.
- Increased levels of phosphate in the body
- Acromegaly
- Reaction to the medicine you take to relax, causing breathing problems or low blood pressure
- Palpation
Related Products
Usage: q.d.
Additional information:
9 of 10
Votes: 328 votes
Total customer reviews: 328
Customer Reviews
Milok, 24 years: Transcribriform Approach to the Ethmoid Planum Indications this route is commonly adopted for the management of intracranial lesions involving the olfactory groove area, above all meningiomas, or lesions extending to it such as sinonasal malignancies (including esthesioneuroblastoma). It is not a reward from the safety professional or recognition from the organization. Pathophysiologic differences in cerebral autoregulation after subarachnoid haemorrhage. Because bleeding abnormalities are noted early in patients with cerebral injuries and facial fractures, replacement of depleted coagulation factors is based on an assessment of coagulation factors in hemorrhaging patients.
Basir, 33 years: It was my first real job out of college, and I had dreamed of working there since I toured the facility while in school. The demonstration ensured that they under stood the language, that the beaking method was physically possible for all the participants, and that, after the lights were turned out, the beaking method was effective in enabling them to remove gloves without contam inating hands. Behavior is and should always remain the keystone of any plan and desired outcome. Sites of involvement differ among adults and children: 90% of pediatric disease is localized within the cranium, with infratentorial involvement (eg, founh ventricle) occurring most commonly among children under the age of 3.
Abe, 65 years: Precipitant stimuli (eg, pain, gastric distention, urinary retention, constipation) should be managed aggressively; the approach should include adequate analgesia and pain control, consideration of nasogastric tube insertion for gastric decompression of gastric atony and paralytic ileus that may occur following autonomic dysfunction, and urinary catheterization to treat bladder atony and urinary retention. Traumatic Brain Injury and Coagulopathy Coagulopathy can be preexisting, usually from medication, or can actually be induced by the severity of the brain injury. Surgical management of primary central nervous system germ cell tumors: proceedings from the Second International Symposium on Central Nervous System Germ Cell Tumors. Endoscopic biopsy ofintraventricular tumors with the use of a ventriculofibcrscope.
Enzo, 39 years: One hundred percent oxygen is then used for ventilation until blood gases can be checked and appropriate adjustments of the F102 made. When the seat belt chime comes on, those in economy class are typically monitored and corrected for standing or going to the restroom. Deep brain stimulation for epilepsy is still being explored, and its place in the armamentarium of epileptologists remains to be determined. The third outcome of punishment is that it addresses only the negative behavior-stop picking your nose!
Contact
0673406227
dppsmyanmar@gmail.com