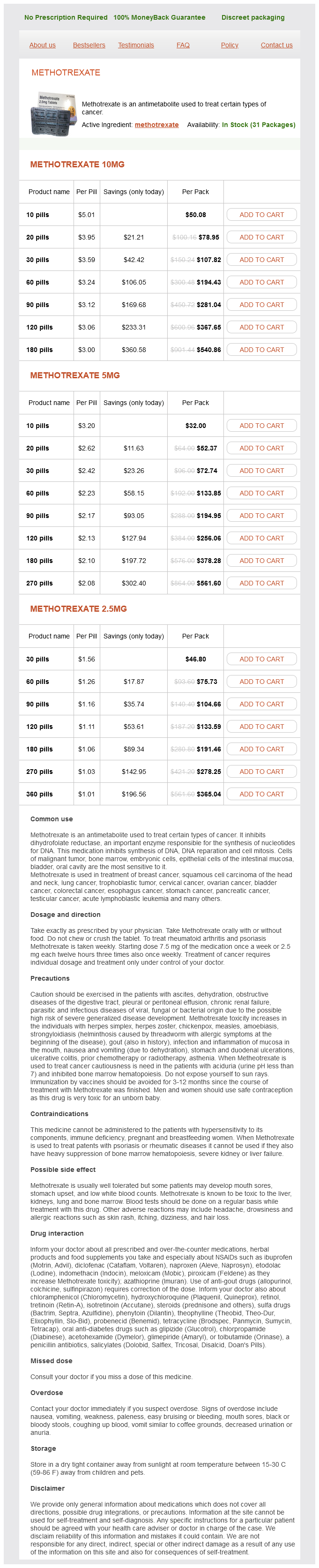
Methotrexate
Methotrexate 10mg
- 10 pills - $50.08
- 20 pills - $78.95
- 30 pills - $107.82
- 60 pills - $194.43
- 90 pills - $281.04
- 120 pills - $367.65
- 180 pills - $540.86
Methotrexate 5mg
- 10 pills - $32.00
- 20 pills - $52.37
- 30 pills - $72.74
- 60 pills - $133.85
- 90 pills - $194.95
- 120 pills - $256.06
- 180 pills - $378.28
- 270 pills - $561.60
Methotrexate 2.5mg
- 30 pills - $46.80
- 60 pills - $75.73
- 90 pills - $104.66
- 120 pills - $133.59
- 180 pills - $191.46
- 270 pills - $278.25
- 360 pills - $365.04
Methotrexate dosages: 10 mg, 5 mg, 2.5 mg
Methotrexate packs: 10 pills, 20 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 741
Only $1.08 per item
Description
The benefits of intervention on seizure control in patients with intractable epilepsy were discussed previously medicine of the wolf methotrexate 2.5 mg buy line. However, it is uncertain if intervention is indicated for patients with nonmedically refractory epilepsy. A prospective populationbased observational study compared conservative versus interventional seizure management [87]. If this is not possible, the pros and cons of all treatment options should be discussed with the patient and, based upon these uncertainties, a decision has to be made. In general, knowledge of having such a lesion results in a decreased quality of life [3]. Some patients show admirable sangfroid in coping with this knowledge; for others, however, their life may be so dominated by the perceived danger that they insist on intervention even when the balance of risks would seem to argue against such a course of action. Another disadvantage of ordering imaging studies in all people with migraine with stereotyped attacks is the cost, discomfort, and risk of the negative investigations in the vast majority. Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Quality of life, anxiety, and depression in patients with an untreated intracranial aneurysm or arteriovenous malformation. Screening families for intracranial aneurysms: anxiety, perceived risk, and informed choice. Psychosocial impact of screening for intracranial aneurysms in relatives with familial subarachnoid hemorrhage. Prevalence of unruptured intracranial aneurysms with emphasis on sex, age, comorbidity, country, and time period: a systematic review and metaanalysis. Incidence and prevalence of intracranial aneurysms and hemorrhage in Olmsted County, Minnesota, 1965 to 1995. Prevalence 9 10 11 12 13 14 15 and risk of rupture of intracranial aneurysms: a systematic review. Subarachnoid haemorrhage in first and second degree relatives of patients with subarachnoid haemorrhage. Repeated screening for intracranial aneurysms in familial subarachnoid hemorrhage. Familial subarachnoid hemorrhage: distinctive features and patterns of inheritance. Unruptured intracranial aneurysms in the Familial Intracranial Aneurysm and International Study of Unruptured Intracranial Aneurysms cohorts: differences in References 741 16 17 18 19 20 21 22 23 24 25 26 27 multiplicity and location. Greater rupture risk for familial as compared to sporadic unruptured intracranial aneurysms.
Pinellia cochinchinense (Pinellia Ternata). Methotrexate.
- Dosing considerations for Pinellia Ternata.
- What is Pinellia Ternata?
- How does Pinellia Ternata work?
- Nausea, morning sickness, cough, birth control, influenza (flu), and inflammation.
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97039
Desiccation of the corneal epithelium and subepithelial tissues occurs at or near the limbus medications prednisone 2.5 mg methotrexate buy with amex, adjacent to conjunctival surface elevations such as those produced after recession resection surgery or in the presence of large filtration blebs. Normal blinking does not wet the involved area properly because the tear film is interrupted by these surface elevations. Patching followed by frequent topical lubrication is most effective in rapidly restoring stromal hydration, although resolution of conjunctival chemosis or bleb revision may be necessary for permanent resolution of dellen. Limbal Stem Cell Deficiency the ocular surface comprises populations of epithelial cells, which are replaced throughout life via proliferation of a distinct subpopulation of cells known as stem cells. Corneal stem cells are located in the basal cell layer of the limbus, whereas conjunctival stem cells may be uniformly distributed throughout the bulbar surface or located in the fornices. Stem cells have an unlimited capacity for self-renewal and are slow cycling (ie, they have low mitotic activity). Transit-amplifying cells, which have a limited capacity for self-renewal, can be found at the limbus as well as at the basal layer of the corneal epithelium. Corneal and conjunctival stem cells can be identified only by indirect means, such as clonal expansion and identification of slow cycling. Approximately 25%33% of the limbus must be intact to ensure normal ocular resurfacing. The normal limbus acts as a barrier against corneal vascularization from the conjunctiva and invasion of conjunctival cells from the bulbar surface. The absence of limbal stem cells reduces the effectiveness of epithelial wound healing, as evidenced by compromised ocular surface integrity with an irregular ocular surface and recurrent epithelial breakdown. Secondary causes include chemical burns, thermal burns, radiation, contact lens wear, ocular surgery, immune-based mucous membrane conjunctivitis (eg, mucous membrane pemphigoid, Stevens-Johnson syndrome), mucous membrane conjunctivitis related to infection (eg, trachoma), pterygia, long-term use of topical medications (pilocarpine, -blockers, antibiotics, antimetabolites), and dysplastic or neoplastic lesions of the limbus. Affected patients usually have recurrent ulceration and decreased vision as a result of the irregular corneal surface. A whorl-like irregularity of the ocular surface is seen following instillation of topical fluorescein. In these cases, treatment with topical corticosteroids is advocated by some clinicians. If the stem cell deficiency is sectoral and mild, the abnormal epithelium can be debrided, allowing for resurfacing of the denuded area with cells derived from the remaining intact limbal epithelium. In more extensive or severe cases of limbal stem cell deficiency, initial therapy with a scleral contact lens may be helpful. If this is not effective, replacement of stem cells by limbal transplantation is an alternative. When the limbus is focally affected in 1 eye (eg, pterygium), a limbal or conjunctival autograft can be harvested from the same eye. For unilateral, moderate or severe chemical injuries, a limbal autograft can be obtained from the healthy fellow eye. For bilateral limbal deficiency, as with Stevens-Johnson syndrome or bilateral chemical burns, a limbal allograft from a human leukocyte antigenmatched living related donor (or, if unavailable, an eye bank donor eye) can be considered; however, systemic immunosuppression is required following limbal allograft transplantation (see the discussion of ocular surface surgery in Chapter 13).
Specifications/Details
Also treatment pancreatitis methotrexate 2.5 mg order without a prescription, the reasons why patients are lost to followup may be related to their outcome. For example, if dead patients are lost to followup, this biases the prognostic data in a favorable direction, and if patients who have made a good recovery (and are mobile) are lost because they move away, this biases the prognostic data in the opposite direction (see Table 10. Furthermore, if not all patients are followed up, the reported prognosis is likely to be overly influenced by the outcome of the last few patients who are remembered most vividly. Random errors and small samples: If the estimate of the outcome is based on the followup of too few patients, it may differ from that in published studies simply by chance alone. Differences in management: Patients may be managed more or less effectively than those in published studies, and thus the outcomes may be better or worse. However, the likely impact of differences in treatment between centers is likely to be swamped by other factors that have a much greater influence on outcome. The differences in outcome between your service and those of your colleagues in other hospitals are more likely to reflect differences in the patients you treat than any differences in the quality of care you provide. It is also difficult to decide on the acceptable accuracy of any predictive tool, because this depends on the consequences, or cost, of getting it wrong. Taking an extreme example: If the clinician was sure that a patient with an apparently severe stroke who was being supported on a ventilator was not going to have an acceptable longterm quality of life, then they 464 10 A practical approach to the management of patients Table 10. Predicting early death Failure to describe adequately the group of patients in whom the work was done Use of unrepresentative cohorts of patients. These clinical features in combination with radiological features such as massive intracerebral hemorrhage with mass effect can help guide management decisions [12, 38]. However, many patients who die do not have these features, and occasionally patients with more than one of these features make an unexpectedly good recovery. Predicting longer term outcomes might withdraw ventilatory support, particularly if the patient had an appropriate advanced directive. However, in this situation the clinician would have to be very confident of their prediction [12]. Unfortunately, methodological problems have so far limited the usefulness of these studies [12, 3537] (Table 10. Many of the factors that predict a high early risk of death also predict a high risk of longterm dependency if the patient survives. In predicting longer term outcome, there is also the problem that further events which may be related to the initial stroke. Methods of prediction A variety of different approaches have been taken in predicting outcome after stroke. The singlefactor approach the simplest method is to identify a single factor, the presence or absence of which early after the stroke indicates the likelihood that the patient will have a good or bad outcome. The most widely used examples are age, severity of the neurological deficit, reduced level of consciousness, or lesion size, which have each been related to poor survival and functional outcome [12, 38]. Although such models are simple to use, and can guide clinical management, the user must be aware of their inaccuracy.
Syndromes
- Arrive at a certain time for the procedure
- Ask your health care provider which drugs you should still take on the day of your surgery.
- Loss of appetite
- There is always a slight chance of infection when the skin is broken.
- Numbness
- When did you first notice this?
- Metabolic abnormalities such as low blood glucose
- Some of these drugs are aspirin, ibuprofen (Advil, Motrin), and naproxen (Aleve, Naprosyn).
- Passage of 10 - 20 stools per day
Related Products
Usage: p.r.n.
Additional information:
10 of 10
Votes: 272 votes
Total customer reviews: 272
Customer Reviews
Ali, 47 years: Rehabilitation stroke units Several trials have indicated benefit from rehabilitation units that admit patients a few days after stroke onset and continue rehabilitation for several weeks.
Volkar, 40 years: Family support 121 122 123 124 125 126 127 128 129 130 131 132 133 134 for stroke: a randomised controlled trial.
Kliff, 50 years: Thus, a patient may reach their optimal functional recovery some months after a stroke and then deteriorate due to progression of a comorbid condition.
Pedar, 26 years: Observational data suggest that both high and low blood pressures early after acute stroke are independently associated with poor outcome (Section 11.
Masil, 25 years: In fact, independently from the etiologic type of dementia diagnosed, a history of stroke confers approximately a double risk of dementia incidence in subjects aged 65 years or more, and this association is not explained by demographic or cardiovascular risk factors and is greater in those with more recent stroke [4].
Peer, 58 years: The accumulation of ferric ions causes signal loss (black), due to a paramagnetic effect, over the entire pial surface (arrows), and in the acoustic nerves (arrowheads).
Contact
0673406227
dppsmyanmar@gmail.com