Metformin
Metformin 850mg
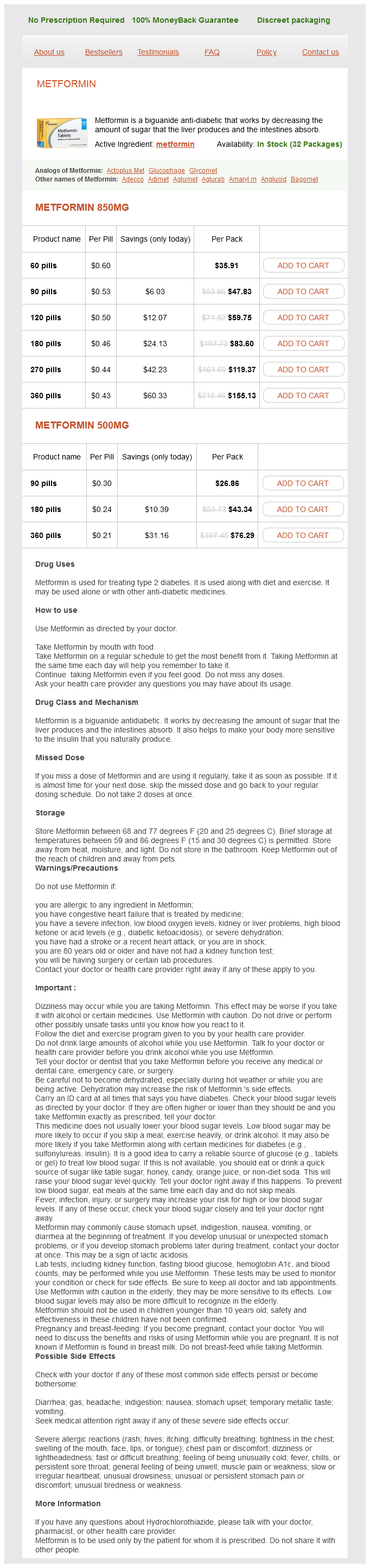
- 60 pills - $35.91
- 90 pills - $47.83
- 120 pills - $59.75
- 180 pills - $83.60
- 270 pills - $119.37
- 360 pills - $155.13
Metformin 500mg
- 90 pills - $26.86
- 180 pills - $43.34
- 360 pills - $76.29
Metformin dosages: 850 mg, 500 mg
Metformin packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 719
Only $0.23 per item
Description
Review of 253 cases of significant pathology in 7 diabetes medications in pill form order 500 mg metformin,910 cholecystectomies in Hong Kong. Histological study of gallbladder and bile duct epithelia in patients with anomalous arrangement of the pancreaticobiliary ductal system: comparison between those with and without a dilated common bile duct. Choledochal cyst and associated malignant tumors in adults: a multicenter survey in South Korea. Immunophenotypic characteristics and classification of non-tumoral (flat) gallbladder dysplasia. Geographic differences of frequency and associations with invasive carcinoma in the two distinct carcinogenetic pathways (conventional dysplasia versus tumoral intraepithelial neoplasia) in the gallbladder. Biotin-rich intranuclear inclusions in morule-lacking adenocarcinoma of the gallbladder: a new category of "neoplastic/non-morular" lesions. Intraductal tubulo-papillary neoplasms of the bile ducts: clinicopathologic, immunohistochemical, and molecular analysis of 20 cases. Tubular adenoma of the gallbladder with squamoid spindle cell metaplasia: report of three cases with immunohistochemical study. Comparative genetic analysis of invasion-resistant (complex non-mucinous pyloric) and invasionprone types of intracholecystic papillary-tubular neoplasms of the gallbladder. Gallbladder adenomas have molecular abnormalities different from those present in gallbladder carcinomas. Mutation and altered expression of beta-catenin during gallbladder carcinogenesis. Histological and genetic changes in malignant transformation of gallbladder adenoma. Mucinous cystic tumors of the pancreas: clinicopathological features, prognosis, and relationship to other mucinous cystic tumors. Hepatobiliary cystadenoma and cystadenocarcinoma: a light microscopic and immunohistochemical study of 70 patients. Biliary tract cancer incidence in the United States: demographic and temporal variations by anatomic site. Cancer facts and figures: estimated new cancer cases and deaths, United States, 2013. Tumor characteristics and survival analysis of incidental versus suspected gallbladder carcinoma. Gallstones and gallbladder cancervolume and weight of gallstones are associated with gallbladder cancer: a case-control study. Multiple carcinomata associated with anomalous arrangement of the biliary and pancreatic duct system: a report of two cases with a literature survey.
Alchemilla. Metformin.
- Is Alchemilla effective?
- How does Alchemilla work?
- Are there safety concerns?
- What is Alchemilla?
- Diarrhea, skin conditions such as ulcers, eczema, and rashes, diabetes, menstrual irregularities, bleeding and wound healing, stomach disorders, muscle spasms, and others.
- Dosing considerations for Alchemilla.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96644
C diabetes mellitus reading 500 mg metformin amex, In the later stages, collagen fibres are deposited within the sinusoidal spaces and hepatic venules, resulting in sinusoidal fibrosis in zone 3 and fibrous obliteration of the small hepatic venules. Hepatocyte atrophy is also present, and congestion is seen at the periphery of the scarring (zone 2). D, Later stage with advanced bridging fibrosis in addition to more recent necrosis and hepatocyte dropout. Remnant hepatic veins/venules are outlined by darker-blue collagen, and sinusoidal dilation is prominent because of the venous outflow obstruction. Extramedullary haematopoiesis in the sinusoids may be seen in myeloproliferative disorders or other diseases that invade and destroy the bone marrow. Nonhaematological neoplasia primary to the liver may also infiltrate the sinusoids, especially those of vascular origin, such as epithelioid haemangioendothelioma303,304 and angiosarcoma (see Chapter 13). Other cellular infiltration within the sinusoids includes rare disorders such as RosaiDorfman disease (sinus histiocytosis with massive lymphadenopathy), Langerhans cell histiocytosis and mastocytosis. Amyloidosis and light-chain deposition disease Hepatomegaly, cholestasis, portal hypertension, ascites and/or liver failure may be the clinical presentation in patients with amyloidosis involving the liver. Acellular and dense deposition of amyloid material along the perisinusoidal space is the characteristic finding. The hepatocellular cords may appear atrophic, and bile plugs may be noted between remaining hepatocytes. In addition to deposition within the sinusoidal spaces, amyloid may also deposit in the arterial wall, portal tracts or liver parenchyma,308310 as well as in the subepithelial spaces of bile ducts and peribiliary glands. However, in the 1990s, convincing evidence of an acquired (thrombotic) aetiology was provided, supported by the common occurrence of infection321 (see next section). Wanless, these conditions have been divided into categories related to pathogenesis and include hypercoagulable states, stasis or mass lesions, vascular injury, surgical manipulation and uncertain mechanisms. In a recent series of 163 patients, median age at diagnosis was 38 years, and 57% of patients were female. Direct x-ray venography, an invasive procedure, is useful to establish the diagnosis in difficult cases and precisely determine obstructive lesions before treatment. There is obstruction of the three hepatic veins by fresh thrombi, one of which protrudes into the lumen of the inferior vena cava (arrow). Periportal regions are spared and demonstrate features of regeneration, such as thickened cell plates. Over time, the venous thrombi become organized and may recanalize, leaving intimal fibrosis (often in the form of multiple layers), delicate webs or multiple lumina. Regeneration of the hepatic parenchyma in regions with relatively spared venous drainage may result in diffuse segmental or lobar hyperplasia.
Specifications/Details
Inflammatory pseudotumours Masses mimicking carcinoma may sometimes be formed by extensive myofibroblastic proliferation resulting from inflammatory injury blood glucose 68 fasting purchase metformin 500 mg mastercard. Patients with PeutzJeghers syndrome and Cowden disease may develop hamartomatous polyps, histologically showing disorganized epithelial proliferation with focal cystic areas. It is well recognized that preinvasive neoplasia in the gallbladder is a precursor to invasive carcinoma as well as an indication of carcinoma elsewhere in the biliary tract. This is based on its usual identification adjacent to invasive carcinomas, its more frequent identification in regions with a higher incidence of gallbladder carcinoma223229 and morphological features recognizable as neoplasia analogous to that occurring in other organs. Fortunately, even highgrade dysplasia/carcinoma in situ is associated with a 90% 10-year survival,30,230232 if invasive carcinoma is definitively excluded by total sampling of the gallbladder. The prognosis is less favourable when the process involves RokitanskyAschoff sinuses. A two-tiered system (low and high grade) is employed for grading gallbladder dysplasia. The two-tiered approach is not only more practical but also more reflective of the biological behaviour, and it parallels a similar two-tiered system recently applied to pancreatic precursor lesions (about which more is known). This patch of basophilic epithelium in otherwise normal mucosa may mimic dysplasia. Much of the basophilia here is attributable to nuclear crowding and overlapping rather than hyperchromasia of individual nuclei. Evaluation of additional tissue sections (typically four additional blocks with multiple tissue portions each) has been advocated to help in the differential of low-grade dysplasia versus reactive changes. These can closely mimic dysplasia because they show crowding and stratification of nuclei and brisk mitotic activity. Characteristic findings that allow the recognition of these lesions as reactive atypia include the presence of maturation toward the surface, similar to the criteria in Barrett oesophagus, and accompanying stromal changes (either capillarization or subtle fibrosis), which in some cases form a band in the surface similar to the pattern in collagenous colitis. Often, intercellular spaces are accentuated, forming clefts, which are regarded as a sign of cell maturity and alignment. Additionally, although they form basophilic zones and nuclear molding/overlapping contributes to their densely basophilic appearance, the nuclei that are individually identifiable often show pale, uniform chromatin. They also often form intracytoplasmic vacuoles as well as a syncytial arrangement that creates a pattern of architectural complexity. In fact, atypia of healing erosion typically shows significant mitotic activity and a high Ki-67 labelling index. Differential diagnosis Dysplasia versus reactive atypia Marked cytological epithelial atypia may be observed in the gallbladder secondary to a variety of insults. The difficulty presented by the morphological similarities between reactive atypia and dysplasia is magnified by the close association of true dysplasia in the gallbladder with longstanding inflammation, injury and repair.
Syndromes
- Pseudoephedrine (Sudafed)
- Medications (cause a syndrome similar to meningitis)
- Inflammation of exposed areas (redness, tenderness, swelling, bleeding)
- Tolbutamide (Orinase)
- Prolonged diarrhea
- Riboflavin
- Cysts in the liver, pancreas, and testes
- Sodium thiosulfate
Related Products
Usage: q.h.
Additional information:
8 of 10
Votes: 205 votes
Total customer reviews: 205
Customer Reviews
Dennis, 50 years: Association between vaccine refusal and vaccine-preventable diseases in the United States: a review of measles and pertussis. These survival factors downregulate or inhibit the intracellular apoptotic signalling pathways at a number of points. Occasionally, a severe focal injury to the liver results in changes histologically indistinguishable from cirrhosis on percutaneous needle biopsy; this focal change is not considered true cirrhosis.
Alima, 52 years: Two major histological patterns of ischaemic liver disease can be distinguished, centrilobular ischaemic necrosis and hepatic infarction. Assessment of liver fibrosis using transient elastography in patients with alcoholic liver disease. The effectiveness of annual versus biennial mass chemotherapy in reducing morbidity due to schistosomiasis: a prospective study in Gezira-Managil, Sudan.
Irmak, 56 years: As cirrhosis develops, there is increasingly diffuse nodularity and obvious fibrous scarring. Pepper424 was first to observe fatty liver in a diabetic patient in 1884, and in 1938, Charles Connor425 described the histopathological features of fatty liver disease in diabetic patients and its association with cirrhosis development, highlighting an aetiological link. In the case of apoptosis (or formation of acidophilic bodies), T lymphocytes likely play a role.
Contact
0673406227
dppsmyanmar@gmail.com