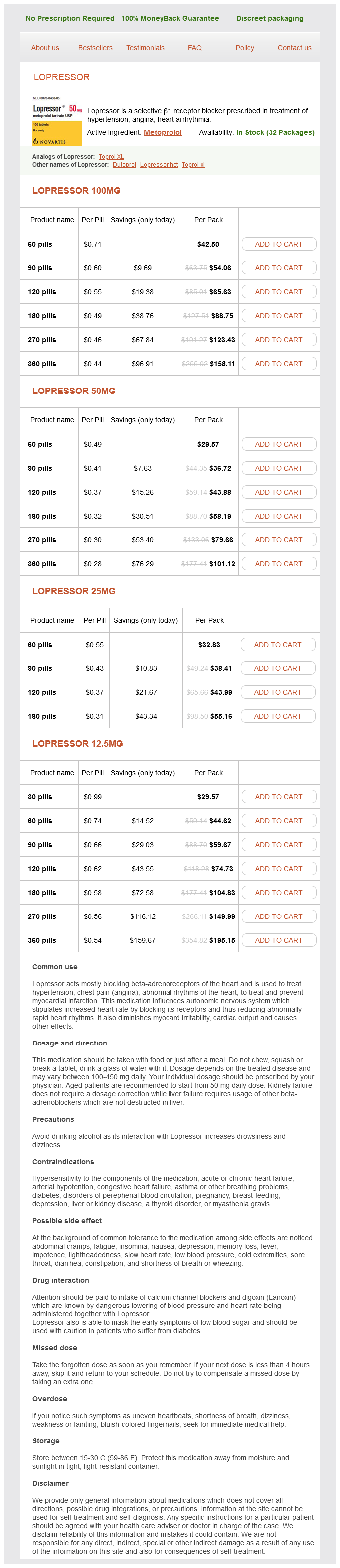
Lopressor
Lopressor 100mg
- 60 pills - $42.50
- 90 pills - $54.06
- 120 pills - $65.63
- 180 pills - $88.75
- 270 pills - $123.43
- 360 pills - $158.11
Lopressor 50mg
- 60 pills - $29.57
- 90 pills - $36.72
- 120 pills - $43.88
- 180 pills - $58.19
- 270 pills - $79.66
- 360 pills - $101.12
Lopressor 25mg
- 60 pills - $32.83
- 90 pills - $38.41
- 120 pills - $43.99
- 180 pills - $55.16
Lopressor 12.5mg
- 30 pills - $29.57
- 60 pills - $44.62
- 90 pills - $59.67
- 120 pills - $74.73
- 180 pills - $104.83
- 270 pills - $149.99
- 360 pills - $195.15
Lopressor dosages: 100 mg, 50 mg, 25 mg, 12.5 mg
Lopressor packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills, 30 pills
In stock: 661
Only $0.58 per item
Description
A, During normal embryogenesis, the fonticulus nasofrontalis forms between the frontal and nasal bones; the prenasal space forms between the nasal bone and nasal cartilage pulse pressure measurement buy lopressor 25 mg low price. B, A tongue of dura extends through the foramen cecum toward the midline nasal skin. Later, this tongue of dura is obliterated and the anterior cranial base is formed; the foramen cecum remains as a vestige of this embryonic tract. C, Abnormal dysjunction during closure of the anterior neuropore leaves a tract of cutaneous ectoderm between the commissural plate and the midline nasal skin. Formation of the anterior frontobasal structures results in a tract whose cutaneous opening may be located at the fonticulus nasofrontalis or anywhere along the dorsum of the nose and that extends through the foramen cecum, between the two halves of a bifid crista galli, and along the anterior cranial base; in rare instances, the tract extends all the way to the commissural plate. Simultaneously, nasal bones develop along the nasal spine and are separated from the frontal bones by a fibrous capsule, the fonticulus nasofrontalis. The nasal spine is separated from the deeper nasal cartilaginous capsule by the prenasal space. During normal embryogenesis, a tongue of dura extends ventrally from the inferior aspect of the anterior cranial fossa and is interposed anteriorly between the frontal and nasal bones at the fonticulus nasofrontalis and inferiorly between the prenasal cartilage and the nasal bones within the prenasal space. During normal development, this dural reflection becomes surrounded by ossifying bone and regresses; remnants of the tract persist as the foramen cecum along the floor of the anterior cranial fossa, between the insertion of the falx cerebri anteriorly and the crista galli posteriorly. When they extend intracranially, they pass through the foramen cecum and typically end within the falx; on rare occasion the tract extends entirely through the falx and travels within the subarachnoid space to end at the lamina terminalis (the site of the anterior neuropore) as predicted embryologically. A malformation involving the cranial rim of the neuropore produces a tract that remains anteriorly located and in close association with the anterior cranial structures. Finally, dermal sinuses are also common in the occipital region,87,88 where they arise from either the roof of the fourth ventricle, the cerebellar vermis, or the subdural space posterior to the cerebellum. The tract may extend either beneath the tentorium into the posterior fossa or above the tentorium toward the occipital lobe or branch to involve both compartments. Although some authors have suggested that occipital dermal sinuses arise from the region of the anterior neuropore,87 this is inconsistent with the association of occipital dermal sinuses with structures derived from the dorsal aspect of the rhombencephalon (cerebellum and fourth ventricle) well distant from the lamina terminalis. Occipital dermal sinuses more likely arise from the rhombencephalic neural tube during neural tube closure. Why dermal sinuses have a predilection for this region of the neuraxis is unclear. The rhombencephalon in humans is among the first regions of the neural tube to undergo neural fold fusion and may therefore be particularly vulnerable to disorders of neurulation; in addition, the presence of the pontine flexure may lend additional physical stress to the neural tube at this site. Finally, the frequent occurrence of dermal sinuses may simply reflect the relatively large size of this region of the neural tube at the time of neurulation. Variably described as the "split notochord syndrome,"89 "endodermal-ectodermal adhesion syndrome,"90 "accessory neurenteric canal syndrome,"91 or "disordered midline integration during gastrulation" syndrome,1 the embryogenesis of these disorders is fully discussed by Dias and Walker. All have in common a splitting of the neuroectoderm into two parts over a portion of its length.
Damiana leaf (Damiana). Lopressor.
- Are there safety concerns?
- What is Damiana?
- Dosing considerations for Damiana.
- Headaches, bedwetting, depression, nervous stomach, constipation, sexual problems, boosting mental and physical stamina, and other conditions.
- Are there any interactions with medications?
- How does Damiana work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96689
This promises to resolve a century-old battle of opinion regarding the routine matter of a treatable nerve entrapment-simply because it is now possible to observe abnormalities on a diagnostic image and correlate them with the clinical picture hypertension diabetes discount lopressor 25 mg buy on line. Imaging results can also be used to guide further definitive testing and percutaneous treatment. Moreover, open magnetic resonanceguided injection procedures provide ready access to virtually any nerve in the body at any point along the nerve to administer precisely targeted blocks and treatment agents for evaluation of nerve compression and possible pain generators. Preoperative neurography (Pre-Op) shows a kink distorting the course of the lower trunk of the brachial plexus. To provide detailed control of such devices, new surgical techniques for deployment of the severed nerve in severed limbs have emerged. The advent of new nerve reconstruction techniques and new minimal-access surgical methods has also raised the bar for what must be learned by a neurosurgeon who wants to be fully skilled and competent in this field. Targeted reinnervation for enhanced prosthetic arm function in a woman with a proximal amputation: a case study. However, not all patients with injured nerves regain useful, let alone full use of their extremities. In this chapter we discuss some of the important clinical pathophysiologic and neurobiologic aspects of nerve injury and regeneration with regard to their role in recovery of limb function after nerve injury or lack thereof. The physical appearance of a sharply transected nerve differs from that of a nerve that has sustained blunt transection changes over time. After sharp transection, the epineurium is cut cleanly, and there is minimal contusive change or hemorrhage in either stump. With time, the stumps of the cleanly cut nerve retract and become enveloped in scar. The amount of proximal neuroma and distal nerve stump scarring is much less than that formed in a more contusive or blunt transection. Blunt transection is associated with a ragged tear of the epineurium acutely and an irregular, longitudinal extent of damage to a segment of the nerve. Bruising and hemorrhage can extend for several centimeters up or down either stump. Retraction and proliferative scarring around the stumps are often more severe than that are seen with sharp transection. Nerve injuries caused by transection, contusion, stretch, traction, and avulsion are generally sustained when medium- to high-energy force is applied directly or indirectly to nerves, whereas injuries such as compressive neuropathy tend to occur when nerves are subjected to chronic or repetitive lowenergy force. Nerve injuries from injection and from radiation and thermal energy involve a rather heterogeneous combination of different injuring factors and can be grouped together as a complex group of nerve injuries.
Specifications/Details
For a ganglion cyst that is extrinsic to and causes compression of a nerve, the involved nerve is protected while the cyst is dissected away, then dissection is performed around the cyst quercetin and blood pressure medication cheap 50 mg lopressor amex. Most ganglia, which are extrinsic to nerve, can be resected in this fashion with preservation of neurological function. The ganglion cyst is usually dissected out, and an internal neurolysis of the involved nerve is performed in the process. As in the extrinsic ganglia, the entry point is isolated and ligated to reduce recurrence. For larger intraneural cysts, the synovium-like contents of the cyst are evacuated, and the capsule is then dissected away from the decompressed and split-apart fascicles. In our experience, most ganglion cysts (61%) arose from the lower extremity, whereas 12% occurred in the brachial plexus region. Common sites of occurrence of this tumor that do not involve nerve include the skin, breast, tongue, larynx, bronchi, and submucosal layer of the gastrointestinal tract. Although this tumor is categorized here as benign, myoblastomas can occasionally assume malignant characteristics. These tumors consist of a mixture of plump, angular cells with cytoplasm containing eosinophilic granules, which represent a large number of lysosomes. When these tumors involve the nerve, they are adherent and require careful dissection for their removal. Treatment involves a wide surgical exposure to determine normal anatomy distal and proximal to the lesion before skeletonizing the involved nerve and moving it away from the lesion. The surgical excision for these tumors is the same as that described for the myoblastoma. Of the two lymphangiomas shown in Table 244-4, one in an upper extremity involved the medial portion of the upper arm, enveloped the proximal median and ulnar nerves, and these nerves required neurolysis. The first rib was resected, and the tumor was successfully removed from the C7, C8, and T1 spinal nerves as well as from the middle and lower trunks of the brachial plexus. Lipomas There are four lipomatous conditions that can affect nerve: a solitary lipoma; a "macrodystrophia lipomatosa," which produces an overgrowth of the hand or fingers and can cause neural compression; an encapsulated lipoma; and a lipofibromatous hamartoma. The usual fatty tumors are benign, subcutaneous, and globose or ovoid, and they usually do not involve nerves. Exceptions occur when a large subcutaneous lipoma envelops or compresses a nerve or originates at a deeper level in the limb and entraps and compresses a nerve. These lipomas can grow quite large and can lie atop or adjacent to the nerve, sometimes surrounding the nerve. Removal is difficult if the lipoma occurs at a plexus level, especially if there has been a prior unsuccessful surgical attempt with resulting scar tissue. The usual management for removal of lipohamartomas, which tend to involve the median nerve at the palmar and sometimes wrist level, is to section the transverse carpal ligament and decompress rather than attempt to remove the lipomatous tissue. An internal neurolysis can be performed, with reduction of the bulk of the tumor from around individual fascicles or, in the case of a more focal lipohamartoma, resection and repair. In our series, 12 lipomas found to compress a nerve were removed from various locations (see Table 244-4).
Syndromes
- A hole in the tissue that divides the sides of the nose (septum)
- Cancerous tumors may cause further complications, including spread to other organs (metastasis).
- Did you fall or twist your ankle recently?
- Coughing up large amounts of blood
- Trim nails after bathing, when they are softer.
- Diverticula
- Deafness
- Obesity
Related Products
Usage: q._h.
Additional information:
9 of 10
Votes: 302 votes
Total customer reviews: 302
Customer Reviews
Grim, 30 years: If the impression can be reduced, a posterior occipitocervical stabilization procedure can then be performed to maintain the reduction. The presence of two separate notochordal anlagen during formation of the notochordal process has never been directly observed, but knockout mice lacking genes for intercalation develop two heminotochords that are not fused in the midline. The patient is then transported to the postoperative care unit with supplemental oxygen and standard monitors. Primary arachnoid cysts are congenital cysts lined by a single layer of flattened, arachnoid cells in a vascular collagenous membrane that lies entirely within the arachnoid layer.
Vatras, 61 years: Because the more proximal nerve comes off the medial cord, it is larger in caliber and has been used as a single trunk graft for repair of axillary and other nerve injuries. Several imaging studies have been useful in identifying these infants with synostosis. Anatomically, a wrist splint places the wrist in the neutral position, which has been shown to create the least amount of pressure or friction, or both, within the carpal tunnel. Neural tube defects: a review of human and animal studies on the etiology of neural tube defects.
Baldar, 46 years: The proximal stump undergoes dieback degeneration, which in human injuries with great force may be a centimeter or more. Vascular symptoms such as intermittent attacks of altered consciousness, transient loss of visual fields, confusion, and vertigo appear in 15% to 25% of patients with abnormalities of the craniovertebral junction. This study was closed after an interim analysis demonstrated a significant increase in relapse rates in patients randomized to the low-dose regimen. No treatment during the neonatal period was necessary, and no complication was observed for the mural fistulas.
Flint, 33 years: Patients with spasticity of cerebral origin showed the least improvement and highest complication rate. This scenario is illustrated by the case of a 10-year-old boy who suffered a flexion injury and was found to have an asymmetric central cord syndrome with a radiograph showing a kyphotic deformity of 8 degrees and horizontal displacement of 2 mm at C4-5. This comprehensive review of the existing literature on ablative techniques for noncancer pain was aimed at summarizing the extent and quality supporting these techniques. Major symptoms persisted in 6% of patients, and complications included wound infections, reflex sympathetic dystrophy, and hematoma.
Urkrass, 41 years: Some of these works have been completed with the creative drawings of Ahmet Sinav, M. As previously discussed, hydrocephalus may persist even after tumor removal, ranging in frequency from 24% to 50%. If feasible, sensory branches are identified by their course toward the skin and left intact or used for transfer to gain sensory function. For incompletely resected or progressive lesions, most units use a radiation dose of 54 Gy administered in 30 fractions,28 although this has not been shown to provide an overall survival benefit in this cohort.
Angir, 25 years: Note that a nerve graft functions as a conduit, whose axons are destined to undergo wallerian degeneration as soon as it is removed from its harvest site. This approach avoids operating unnecessarily on patients who are destined to recover spontaneously, and yet it is early enough to avoid permanent changes, such as contractures, in denervated and developing skeletal muscle. In fact, there is no reason why every spinal level could not be subjected to the laminectomy we describe without the need for concomitant spinal stabilization. Recent reports of medical treatment with methylprednisolone and calcitonin have suggested that a new medical option might be used for lesions in areas difficult to excise, such as in the spinal atlas-axis joint.
Contact
0673406227
dppsmyanmar@gmail.com