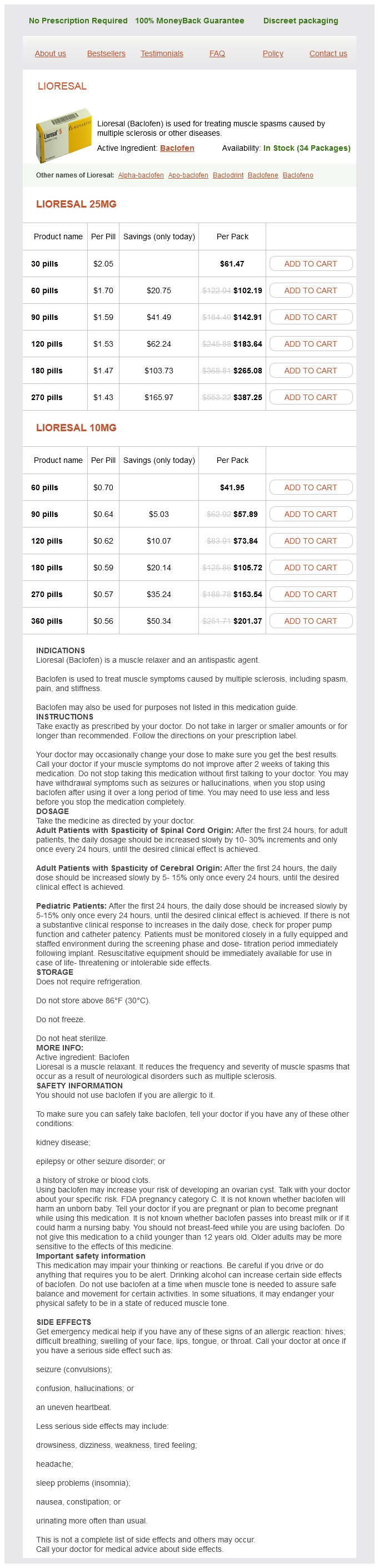
Lioresal
Lioresal 25mg
- 30 pills - $61.47
- 60 pills - $102.19
- 90 pills - $142.91
- 120 pills - $183.64
- 180 pills - $265.08
- 270 pills - $387.25
Lioresal 10mg
- 60 pills - $41.95
- 90 pills - $57.89
- 120 pills - $73.84
- 180 pills - $105.72
- 270 pills - $153.54
- 360 pills - $201.37
Lioresal dosages: 25 mg, 10 mg
Lioresal packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 614
Only $0.59 per item
Description
Fluoroquinolones and -lactam antimicrobials are not considered first-line therapy because of the propensity to induce resistance in gut flora and muscle relaxant uses lioresal 25 mg purchase line, for -lactams, a lower efficacy. A longer course of 7 days is recommended when the duration of symptoms is more than 7 days, for women with an early recurrence of symptomatic infection (<30 days) following prior antimicrobial therapy, and when treatment is with a -lactam antimicrobial. For women with mild to moderate symptoms, about 50% are symptom free by 7 days following initiation of antiinflammatory therapy and without antibiotics. Some women with mild symptoms may choose to delay antimicrobial therapy to see if spontaneous resolution occurs with antiinflammatory medication, but whether to delay antibiotics should be a patient decision. Frequent recurrent acute cystitis is a disruptive and distressing problem for many women. Antimicrobial prophylaxis, given either as a long-term, low-dose regimen or after intercourse, prevents 95% or more of recurrent episodes and is usually recommended for women with two episodes in 6 months or 3 in 1 year (Table 47. Continuous low-dose prophylaxis taken at bedtime is recommended, with an initial course of 6 to 12 months. When prophylactic therapy is discontinued, the frequency of urinary infection is similar to that observed before prophylaxis. Postcoital prophylaxis is, obviously, most appropriate for women who identify sexual intercourse as a precipitating factor for recurrent symptomatic episodes. An alternate approach preferred by some women, especially with less frequent recurrences or who are concerned about developing an infection while traveling, is self-treatment. It is appropriate for women who are compliant with management and reliable in identifying their symptomatic episodes. The most important nonantimicrobial intervention for prevention of recurrent urinary infection is avoidance of spermicide use. The daily intake of cranberry or lingonberry juice or cranberry tablets was previously reported to decrease the frequency of recurrent infection by 30%, but recent blinded placebo-controlled trials have not reported a benefit. Vaccines to prevent recurrent uncomplicated urinary infection and use of probiotics to reestablish normal gut or vaginal flora are being investigated, but studies to date have not shown consistent benefits with either of these approaches. Women who experience acute uncomplicated urinary infection are also at risk for nonobstructive pyelonephritis, with the frequency of episodes of cystitis relative to pyelonephritis reported to be 1829 to 1. Risk factors for developing acute pyelonephritis are similar to those for acute cystitis for premenopausal women; frequency of sexual intercourse is the most important. The P fimbria, an adhesin that attaches to uroepithelial cells and induces an inflammatory response, is the most important virulence factor. Additional organism virulence factors include production of hemolysin, which may lyse host cells, and aerobactin, an iron scavenger that may promote bacterial growth. Acute pyelonephritis presents classically with fever and costovertebral angle pain and tenderness, often associated with lower urinary tract symptoms. A urine specimen for culture and susceptibility testing should be obtained before the initiation of antimicrobial therapy from every woman with a suspected diagnosis of pyelonephritis.
Umbrella Leaves (Butterbur). Lioresal.
- What other names is Butterbur known by?
- What is Butterbur?
- Pain, colic, cough, asthma, irritable bladder, urinary tract spasms, wounds, and other conditions.
- How does Butterbur work?
- Hayfever caused by grass pollen.
- Are there safety concerns?
- Are there any interactions with medications?
- Preventing migraine headaches.
- Dosing considerations for Butterbur.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96639
Unfortunately spasms in throat 10 mg lioresal purchase amex, at 2 years there was no reduction in the rate of late-onset seizures, regardless of early 7-day courses of phenytoin or valproate or 6 months of valproate therapy. However, after hematoma evacuation and intracranial decompression, these injured vessels can begin hemorrhaging. Oftentimes they are contralateral to the side of decompression at the site of contrecoup injury. A number of risk factors for development of hydrocephalus have been reported, including size of the craniectomy, with large craniectomy carrying a higher risk of hydrocephalus. A single episode of hypotension in the absence of hypoxia increased the odds of mortality, and multiple episodes of hypotension had an odds ratio of 8. Hypoxia (PaO2 < 60), which often is associated with hypotension, also increases the risk of mortality and should be avoided at all costs. These imbalances follow the triphasic response thought to arise after injury to the pituitary stalk. Axons from the hypothalamus project in the pituitary stalk through the diaphragm and into the posterior pituitary gland in the sella turcica. During head trauma, the rapid acceleration and deceleration of the brain within the skull can stretch and damage the stalk. This manifests clinically with increasing urine output, increasing serum osmolality, low specific gravity, and hypernatremia. Clinically this presents with hyponatremia and fluid retention, commonly seen from days 5 to 12 after injury. Patients with hyponatremia are managed with fluid restriction, salt tabs, and hypertonic saline. Because the management of the two conditions is directly opposite to one another, close attention must be paid when patients are experiencing this phenomenon, and the three phases should be anticipated to optimize management. The latest Brain Trauma Foundation Guidelines provide a level 3 recommendation for use of mechanical and pharmacological prophylaxis. The risk is around 3% to 12%, depending on the study, although some studies report much higher rates. In addition, breakdown or dehiscence of the wound is difficult treat and can require additional surgeries, even occasionally requiring a free flap for closure. Impaired brain tissue oxygenation can occur secondary to an insufficient systemic hemoglobin level. To prevent this, a small window of decompression is avoided during surgery and the craniectomy is made as large as safely possible. It is characterized by sinking of the flap that occurs in the late stage after hemicraniectomy. Symptomatically, patients can present with acute neurological deficits, such as motor impairment. Should the management of isolated traumatic subarachnoid hemorrhage differ from concussion in the setting of mild traumatic brain injury
Specifications/Details
Careful positioning of the neck and proper placement of a bite block rather than an oropharyngeal airway may reduce this risk muscle spasms xanax withdrawal cheap lioresal 10 mg overnight delivery. Rarely, peripheral neuropathies can result from neurosurgical procedures in the sitting position. The most commonly injured nerve in the sitting position is the common peroneal nerve, resulting in foot drop. Injury to the common peroneal nerve may be due to ischemic compression or from stretching the sciatic nerve. The risk-to-benefit ratio of neurosurgical procedures in the sitting position has been considerably debated. Today, the most common procedure done in the sitting position in the United States is an insertion of a deepbrain stimulator8 or occasionally for difficult-to-access lesions such as pineal tumors. In Europe, the sitting position is still very popular and is the preferred position for surgery of the posterior cranial fossa. Many authors have argued that the fear of catastrophic complications related to the sitting position seems unwarranted. The presence of a right to left intracardiac shunt has generally been considered an absolute contraindication to surgery in the sitting position, although this premise has been challenged in recent years. In the immediate postoperative period, pneumocephalus is common and may persist for weeks after surgery6 (Table 2. Pneumocephalus after surgery in the sitting position may occur with or without the use of nitrous oxide. With extreme head and neck flexion, quadriplegia may result from cervical spine ischemia. Summary the long duration of neurosurgical procedures and the fact that patients are completely covered by drapes makes proper patient positioning especially critical. A comprehensive preoperative assessment is vital, and the position decided on should be communicated to the anesthesiologist and nursing staff as early as possible. Proper patient positioning requires the cooperation and communication between all operating room personnel. Pinning the head may result in significant hypertension and tachycardia and should be anticipated by the anesthesiologist. Prior to pinning, patients should be preemptively treated with an opioid or anesthetic agent, and blood pressure should be carefully monitored during this time. Extreme hyperflexion is discouraged, and at least 23 fingerbreadths should be maintained between the mandibular protuberance and manubrium at all times. Each patient position is associated with unique benefits and risks and should be considered for all neurosurgical patients.
Syndromes
- Isotope study
- Tay-Sachs or other genetic disease
- The puncture site is covered with an adhesive strip to stop any bleeding.
- Damaged or abnormal heart valve
- Trees
- Amount swallowed
- Is breathing rapidly
- Brain herniation (pressure on the brain severe enough to cause coma and death)
Related Products
Usage: q.3h.
Additional information:
10 of 10
Votes: 310 votes
Total customer reviews: 310
Customer Reviews
Phil, 63 years: Analysis of catecholamine and vasoactive peptide release in intracranial arterial venous malformations. The cycler delivers a set number of exchanges over 8 to 10 hours, with the last fill constituting the long day dwell, which may be necessary to provide additional dialysis to achieve solute and fluid removal targets.
Kayor, 31 years: A thorough physical examination may identify underlying systemic diseases that may affect transplant suitability, such as poor dentition or diminished arterial pulses. If a metabolic evaluation is pursued, it is identical for first-time and recurrent stone formers.
Grobock, 26 years: However, some patients will not tolerate an awake procedure, including children, those with extreme anxiety, and those in whom dystonic posturing or other movement disorders preclude proper intraoperative positioning. Special circumstances need to be addressed for patients on clopidogrel or other antiplatelet agents used to manage cardiovascular health.
Treslott, 21 years: Anticoagulation for the prevention of both anastomotic thrombosis and venous thromboembolism remains variable among plastic surgeons and is constantly debated in the literature. In the case of combined procedures, swelling of the temporalis muscle may compress the donor vessel.
Rozhov, 32 years: Although good functional outcomes may result from surgical resection in this group, optimal patient selection remains the key. Hypercalciuria is a characteristic feature of Dent disease and is associated with nephrocalcinosis in most and kidney stones in many patients with Dent disease; nephrocalcinosis and nephrolithiasis are less common in Lowe syndrome.
Yasmin, 48 years: Special attention and coordination between the surgeons and anesthesia team are planned to react expeditiously. Because microcatheters are inserted selectively into small cerebral arteries, patients will receive heparin to reduce catheter-induced thromboembolism.
Contact
0673406227
dppsmyanmar@gmail.com