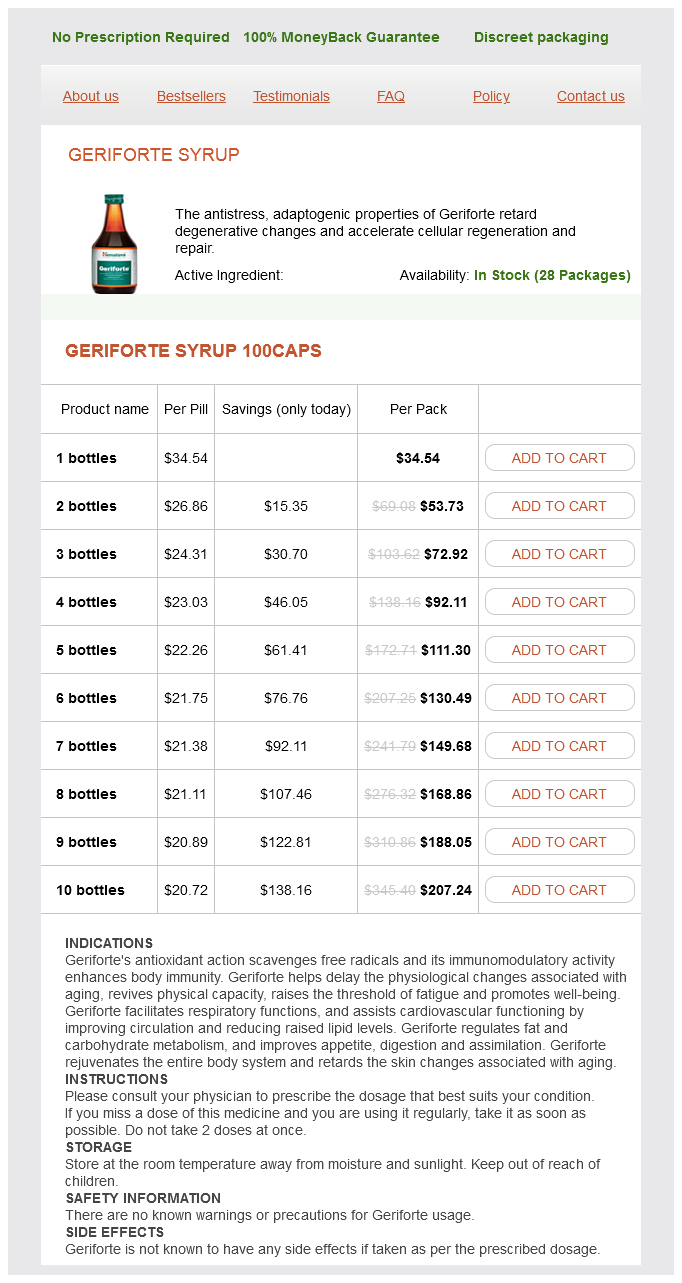
Geriforte Syrup
Geriforte Syrup 100caps
- 1 bottles - $34.54
- 2 bottles - $53.73
- 3 bottles - $72.92
- 4 bottles - $92.11
- 5 bottles - $111.30
- 6 bottles - $130.49
- 7 bottles - $149.68
- 8 bottles - $168.86
- 9 bottles - $188.05
- 10 bottles - $207.24
Geriforte Syrup dosages: 100 caps
Geriforte Syrup packs: 1 bottles, 2 bottles, 3 bottles, 4 bottles, 5 bottles, 6 bottles, 7 bottles, 8 bottles, 9 bottles, 10 bottles
In stock: 653
Only $22.02 per item
Description
I these drugs are unsuccess ul herbals solutions buy cheap geriforte syrup 100 caps on-line, then the addition o other drugs such as topiramate, zonisamide, lacosamide, or tiagabine is indicated. Patients with myoclonic seizures resistant to valproic acid may bene t rom the addition o clonazepam or clobazam, and those with absence seizures may respond to a combination o valproic acid and ethosuximide. For some, surgery can be extremely e ective in substantially reducing seizure requency and even providing complete seizure control. Rather than submitting the patient to years o unsuccess ul medical therapy and the psychosocial trauma and increased mortality associated with ongoing seizures, the patient should have an ef cient but relatively brie attempt at medical therapy and then be re erred or surgical evaluation. The most common surgical procedure or patients with temporal lobe epilepsy involves resection o the anteromedial temporal lobe (temporal lobectomy) or a more limited removal o the underlying hippocampus and amygdala (amygdalohippocampectomy). Focal seizures arising rom extratemporal regions may be abolished by a ocal neocortical resection with precise removal o an identi ed lesion (lesionectomy). When the cortical region cannot be removed, multiple subpial transection, which disrupts intracortical connections, is sometimes used to prevent seizure spread. In some cases, standard noninvasive evaluation is not suf cient to localize the seizure onset zone, and invasive electrophysiologic monitoring, such as implanted depth or subdural electrodes, is required or more de nitive localization. The exact extent o the resection to be undertaken can also be determined by per orming cortical mapping at the time o the surgical procedure, allowing or a tailored resection. This involves electrocorticographic recordings made with electrodes on the sur ace o the brain to identi y the extent o epilepti orm disturbances. I the region to be resected is within or near brain regions suspected o having sensorimotor or language unction, electrical cortical stimulation mapping is per ormed on the awake patient to determine the unction o cortical regions in question in order to avoid resection o so-called eloquent cortex and thereby minimize postsurgical de cits. Advances in presurgical evaluation and microsurgical techniques have led to a steady increase in the success o epilepsy surgery. Clinically signi cant complications o surgery are <5%, and the use o unctional mapping procedures has markedly reduced the neurologic sequelae due to removal or sectioning o brain tissue. For example, about 70% o patients treated with temporal lobectomy will become seizure ree, and another 1525% will have at least a 90% reduction in seizure requency. Marked improvement is also usually seen in patients treated with hemispherectomy or catastrophic seizure disorders due to large hemispheric abnormalities. Postoperatively, patients generally need to remain on antiepileptic drug therapy, but the marked reduction o seizures ollowing resective surgery can have a very bene cial e ect on quality o li. For example, some patients have seizures arising rom more than one location, making the risk o ongoing seizures or potential harm rom the surgery unacceptably high. The duration o seizure activity su cient to meet the de nition o status epilepticus has traditionally been speci ed as 1530 min. However, a more practical de nition is to consider status epilepticus as a situation in which the duration o seizures prompts the acute use o anticonvulsant therapy. Many epilepsy patients are completely normal between seizures and live highly success ul and productive lives. In contrast, patients with seizures secondary to developmental abnormalities or acquired brain injury may have impaired cognitive unction and other neurologic de cits.
Herpestis monniera (Brahmi). Geriforte Syrup.
- Aiding learning and memory improvement.
- Irritable bowel syndrome (IBS).
- Dosing considerations for Brahmi.
- How does Brahmi work?
- Are there any interactions with medications?
- Asthma, backache, hoarseness, mental illness, epilepsy, rheumatism, sexual problems, fluid retention, and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96743
Although these agents do not show comparable e cacy to levodopa herbals sweets 100 caps geriforte syrup free shipping, they are associated with ewer motor complications. It should be noted that even with use o the dopamine agonists, eventual treatment with levodopa is required in most patients. The risk is low overall, but because this patient is untreated, there are other better options or his care. Pain can occur spontaneously, but is o en elicited by light touch or movements o the a ected areas, including chewing, speaking, or smiling. Compression o the trigeminal nerve root by a blood vessel is believed to be the most common cause o trigeminal neuralgia. Diagnosis o trigeminal neuralgia is made based on clinical eatures, and laboratory or radiologic examination is not required. The initial treatment is typically with carbamazepine, which has been demonstrated to be e ective in 50%75% o cases. Most patients require a dose o 200 mg qid or greater, although doses >1200 mg daily con er no added bene t. For patients who do not tolerate carbamazepine, other antiseizure medications have been used to control the symptoms. In cases that are re ractory to medical therapy, microvascular surgical decompression can be considered and has a >70% success rate in relieving pain. Despite an initial success rate o >95%, up to one-third o individuals will have recurrence o symptoms, and the procedure is associated with an increased risk o complications including acial numbness and jaw weakness. The di erential diagnosis o trigeminal neuralgia includes temporal arteritis, migraine or cluster headaches, and multiple sclerosis. Supportive therapy may include use o cough assist devices, invasive or noninvasive ventilatory support, and gastrostomy eeding in addition to a variety o orthopedic assistive devices. This rare disorder has a prevalence o about 25 per 100,000 and is commonly grouped within a category o disorders o atypical parkinsonism that includes progressive supranuclear palsy, corticobasal ganglionic degeneration, and rontotemporal dementia. I that approach ails, other agents including midodrine, ephedrine, pseudoephedrine, or phenylephrine may be used. Conservative treatment o the gastrointestinal and urinary symptoms include requent small meals, stool so eners, bulking agents, and intermittent bladder catheterization. Risk actors or decreased survival include emale R eview and Self-A ssessment arteritis may present with super cial acial pain. One typically also has symptoms including jaw claudication, di use myalgias, and potential visual symptoms. Multiple sclerosis can present with trigeminal neuralgia, but most patients have other symptoms o the disease as well, including weakness or visual symptoms.
Specifications/Details
The mortality rate is <5% in optimal settings; death usually results rom secondary pulmonary complications herbs los gatos cheap 100 caps geriforte syrup. Such axonal damage may be either primary or secondary in nature (see "Pathophysiology," above), but in either case success ul regeneration cannot occur. Other actors that worsen the outlook or recovery are advanced age, a ulminant or severe attack, and a delay in the onset o treatment. Biopsy typically reveals little in ammation and onion-bulb changes (imbricated layers o attenuated Schwann cell processes surrounding an axon) that result rom recurrent demyelination and remyelination. Cases associated with monoclonal IgA or IgG kappa usually respond to treatment as avorably as cases without a monoclonal gammopathy. These neuropathies are sensorimotor, are usually mild and slowly progressive but may be severe, and generally do not reverse with success ul suppression o the myeloma. In contrast, myeloma with osteosclerotic eatures, although representing only 3% o all myelomas, is associated with polyneuropathy in one-hal o cases. The most common pattern is multi ocal (asymmetric) motor-sensory neuropathy (mononeuropathy multiplex) due to ischemic lesions o nerve trunks and roots; however, some cases o vasculitic neuropathy present as a distal, symmetric sensorimotor polyneuropathy. Systemic vasculitis should always be considered when a subacute or chronically evolving mononeuropathy multiplex occurs in conjunction with constitutional symptoms (ever, anorexia, weight loss, loss o energy, malaise, and nonspeci c pains). Diagnosis o suspected vasculitic neuropathy is made by a combined nerve and muscle biopsy, with serial section or skip-serial techniques. Approximately one-third o biopsy-proven cases o vasculitic neuropathy are "nonsystemic" in that the vasculitis appears to a ect only peripheral nerves. Nevertheless, clinically silent involvement o other organs is likely, and vasculitis is requently ound in muscle biopsied at the same time as nerve. Most patients present with isolated sensory symptoms in their distal extremities and have Edx eatures o an axonal sensory or sensorimotor polyneuropathy. They usually do not respond to immunotherapies designed to reduce the concentration o the monoclonal protein. An exception is the syndrome o IgM kappa monoclonal gammopathy associated with an indolent, longstanding, sometimes static sensory neuropathy, requently with tremor and sensory ataxia. In the majority, 690 Vasculitic neuropathy may also be seen as part o the vasculitis syndrome occurring in the course o other connective tissue disorders. Management o these neuropathies, including the "nonsystemic" vasculitic neuropathy, consists o treatment o the underlying condition as well as the aggressive use o glucocorticoids and cyclophosphamide. Use o these immunosuppressive agents has resulted in dramatic improvements in outcome, with 5-year survival rates now greater than 80%. Recent clinical trials ound that the combination o rituximab and glucocorticoids is not in erior to cyclophosphamide and glucocorticoids. The onset is of en asymmetric with dysesthesias and sensory loss in the limbs that soon progress to a ect all limbs, the torso, and the ace. Marked sensory ataxia, pseudoathetosis, and inability to walk, stand, or even sit unsupported are requent eatures and are secondary to the extensive dea erentation.
Syndromes
- LH-releasing hormone (LHRH) analogs
- Low urine output (a sign of decreasing kidney function)
- 40 calories or less per serving
- Peas
- Are pregnant
- Has difficulty seeing
- Children and adolescents who take medications should be followed by a doctor for side effects. Parents or caregivers should watch for suicidal thoughts or behaviors, nervousness, irritability, moodiness, or sleeplessness that is getting worse. Get medical help for these symptoms right away.
- Myxedema
Related Products
Usage: q._h.
Additional information:
8 of 10
Votes: 220 votes
Total customer reviews: 220
Customer Reviews
Gorn, 30 years: I per orated mesh is seen, the tape is removed, and the V needle is again passed through a newly created periurethral tunnel that lies slightly medial to the original. Nerve biopsy can reveal noncaseating granulomas in ltrating the endoneurium, perineurium, and epineurium along with lymphocytic necrotizing angiitis. The presentation o more carcinogenic smoke to the alveolar portions o the lung has resulted in an increase in the risk o lung cancer, and possibly chronic obstructive pulmonary disease, among smokers over the past six decades.
Iomar, 33 years: Stereognosis re ers to the ability to identi y common objects by palpation, recognizing their shape, texture, and size. I there is a paucity o pain and sensory involvement, motor neuron disease should be considered as well. Anemia with stippling o erythrocytes is common, and occasionally pancytopenia and aplastic anemia can develop.
Contact
0673406227
dppsmyanmar@gmail.com