Butenafine
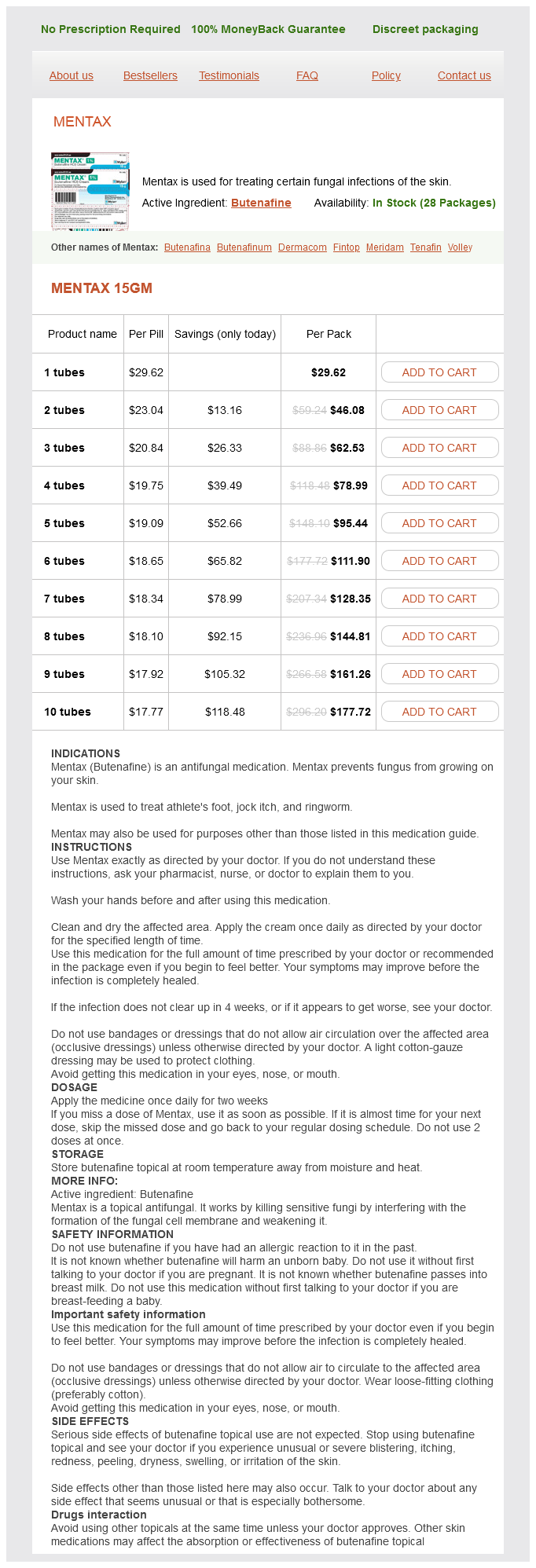
Mentax 15gm
- 1 tubes - $29.62
- 2 tubes - $46.08
- 3 tubes - $62.53
- 4 tubes - $78.99
- 5 tubes - $95.44
- 6 tubes - $111.90
- 7 tubes - $128.35
- 8 tubes - $144.81
- 9 tubes - $161.26
- 10 tubes - $177.72
Butenafine dosages: 15 mg
Butenafine packs: 1 tubes, 2 tubes, 3 tubes, 4 tubes, 5 tubes, 6 tubes, 7 tubes, 8 tubes, 9 tubes, 10 tubes
In stock: 516
Only $18.88 per item
Description
Once the pulmonary artery pressure is lower than the right ventricular pressure fungus gnat off uk discount butenafine 15 mg with visa, the pulmonary valve will open, and antegrade pulmonary blood flow will ensue, with improved left ventricular filling. As in the fetus, the ductus arteriosus plays a pathologic role by limiting antegrade pulmonary blood flow and promoting circular shunting. If prostaglandin therapy is necessary for profound cyanosis, then the neonate should be trialed off as soon as feasible, with close hemodynamic monitoring in the intensive care unit. With intensive medical management and sufficient time for the pulmonary vascular resistance to fall, some neonates, even with severe tricuspid regurgitation and circular shunting at birth, will be able to avoid surgery in the neonatal period. For cases of functional pulmonary atresia where medical management is the first-line therapy, as described previously, there are instances in which the right ventricle has recovered and is ejecting antegrade, but hemodynamic instability persists due to patency of the ductus arteriosus. Occasionally, the neonate is unable to be weaned from support, but the right ventricle is felt to be adequate. However, survival was significantly diminished when anatomic pulmonary atresia was present. An aortopulmonary shunt may be placed to augment pulmonary blood flow, with a biventricular, one-and-a-half ventricular, or univentricular approach pursued later. Alternatively, a right ventricular exclusion procedure, also known as the Starnes procedure, may be performed. This operation involves fenestrated tricuspid valve closure with right atrioplasty and ventriculoplasty and placement of an aortopulmonary shunt with main pulmonary artery ligation. Neonatal hospital survival of 69% was reported by Starnes and colleagues, with survivors proceeding to the Glenn and Fontan operations to complete univentricular palliation. Intermediate-term follow-up demonstrated regression of right ventricular size, creating less septal impingement and normalization of left ventricular systolic function. Therefore, instead of the normal draining of the coronary sinus into the right atrium via its usual orifice, there is a persistence of the wide communication between the sinus venosus and both atria, allowing a left-to-right shunt after birth. Unlike a large coronary sinus receiving a persistent left superior vena cava that eventually drains into the right atrium, this defect allows a communication between the two atria, and the left superior vena cava drains directly into the left atrium. During fetal life, the normal atrial communication at the oval fossa allows right-to-left atrial flow, allowing oxygen-rich blood to flow to the left heart and, consequently, to the brain and the heart. Some time after birth, following the normal decrease in pulmonary pressure and resistance, and immediate increase of systemic vascular resistance caused by the loss of the placenta, the foramen should close and prevent intraatrial shunting. The foraminal mechanism has been found to be substantially less efficient than was previously believed, since the advent of modern postnatal cardiac ultrasound has shown that a substantial number of infants under 6 months of age have intra-atrial left-to-right shunts. When the septum primum is deficient, the right atrial and ventricular pressure decreases gradually as the compliance increases, leading to a predominant left-to-right shunting across the atrial communication.
Nosebleed (Yarrow). Butenafine.
- How does Yarrow work?
- What is Yarrow?
- Fever, common cold, hayfever, diarrhea, stomach discomfort, bloating, gas, toothache, and other conditions.
- Dosing considerations for Yarrow.
- Are there safety concerns?
- Are there any interactions with medications?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96188
Branch pulmonary artery stenosis is another common complication of the arterial switch operation and is less amenable to balloon angioplasty at catheterization fungus gnats damp discount butenafine 15 mg on-line. Finally, arrhythmias, including sinus node disease, can be present in up to 10% of the patients in the long term. From a four-chamber image sweeping toward the fetal head (a) and a sagittal image (b) the aortiorly deviate infundibular septum (arrow) can be seen crowing the subaortic area. Overall survival to the age of 5 has been reported between 70% and 92%, and to the age of 10 years, 64%91%. The pulmonary valve is usually wedged between the atrial septum Transposition of the great arteries and the mitral valve, and there is fibrous continuity between the two mentioned valves. The abnormal twist and relationship of the ventricles vary in degree and may be extreme to the point of causing a superior-inferior relationship of the ventricles (criss-cross heart). Similarly to the normal heart, the anterior descending and circumflex arteries supply the anatomically left ventricle, and the right coronary artery, the morphologic right ventricle. These patients display an in-series circulation with unsaturated blood returning to the right atrium through the systemic veins flowing into the left ventricle and being ejected to the lungs, and saturated blood returning via the pulmonary veins to the left atrium, flowing to the right ventricle, and then being ejected into the aorta to the body. However, in spite of a physiologically corrected circulation, even in patients who have no other associated abnormalities, the natural history and postnatal hemodynamics are quite different from a person with normal anatomy in the short and long term. Depending on the associated cardiac lesions and need for surgical intervention, the evolution of heart failure may be accelerated. A multi-institution study with 182 patients81 showed that by the age of 45%, 67% of the patients with associated lesions and 25% without associated lesions, had systemic ventricular dysfunction and congestive heart failure. The remaining 44 patients underwent an "anatomical repair" (10 had "double-switch" procedure, and 34 had atrial switch plus intraventricular rerouting). This study suggested that late functional outcomes of anatomic repair were superior to physiologic repair,85 but the findings from this study are limited by its retrospective design. Tricuspid valve dysplasia is present in the vast majority of cases and likely contributes to the increased likelihood of valve dysfunction long term. Additionally, the abnormal conduction anatomy results in increasing incidence of congenital heart block with age (roughly 1%2% per year), adding further to the morbidity and mortality risks of the patient. In the majority of cases, there is no critical outflow obstruction; therefore, prostaglandins are not necessary. In the absence of other intracardiac pathology, affected patients can be clinically well for many years and may even go unrecognized until later in life. Furthermore, this procedure is not without risks, including risks associated with atrial baffling83 and risks related to the arterial switch. For many fetuses, the cardiac axis or position is not normal with mesocardia or dextrocardia. This is particularly true of the tricuspid valve, which may be thickened, redundant, and have morphological features of Ebstein anomaly. From the four-chamber view, sweeping cephalad to the ventricular outlets confirms the presence of V-A discordance (Video 29. Long-axis sweeps in a plane that is perpendicular to the ventricular septum from the four-chamber view may demonstrate the parallel relationship of the great arteries.
Specifications/Details
Absence of cystathionine -synthase (cystathionine synthetase) blocks the metabolism of homocysteine antifungal rash cream cheap butenafine 15 mg visa, causing the accumulation of homocystine and methionine. Non-neurological features include ectopia lentis or severe myopia, marfanoid appearance, osteoporosis, pectus excavatum, genu valgum, scoliosis, and cerebral thromboembolism. Intelligence is generally higher in B6responsive than B6-nonresponsive homocystinuria. High plasma homocysteine concentrations adversely affect collagen metabolism and are responsible for intimal thickening of blood vessel walls, leading to arterial and venous thromboembolic disease. Occlusion of the coronary or carotid arteries can lead to sudden death or severe neurological handicap. Dislocation of the lens, an almost constant feature of homocystinuria, typically occurs between 2 and 10 years of age. Older children have osteoporosis, often first affecting the spine resulting in scoliosis. Many children are tall and thin, with blond, sparse, brittle hair and a Marfan syndrome habitus. This habitus does not develop until middle or late childhood and serves as a clue to the diagnosis in fewer than 40% of cases. The diagnosis is suspect in any infant with isolated and unexplained developmental delay, since disease-specific features may not appear until later childhood. The presence of either thromboembolism or lens dislocation strongly suggests homocystinuria. The biochemical features of homocystinuria are increased concentrations of plasma homocystine, total homocysteine, and methionine; increased concentration of urine homocystine; and reduced cystathionine -synthase enzyme activity. Prenatal diagnosis is available for fetuses at risk by measurement of cystathionine -synthase enzyme activity assayed in cultured amniocytes, but not in chorionic villi, since this tissue has low enzyme activity at baseline. All patients with homocystinuria should receive 10 mg/kg/day of pyridoxine, up to a maximum of 500 mg/day for 6 weeks. Plasma tHcy is measured twice before treatment and twice during treatment; the test should not be done if the patient is catabolic. The protein intake should be normal, folate supplements should be given, and vitamin B12 deficiency should be corrected prior to testing. Patients who achieve plasma tHcy levels below 50 mol/L on pyridoxine are clearly B6 responsive and do not need any other treatment. Folate and vitamin B12 optimize the conversion of homocysteine to methionine and help to decrease homocysteine levels. If the tHcy falls more than 20%, but remains above 50 mol/L, additional treatment should be considered. Branched-chain ketoacid dehydrogenase is the enzyme responsible for oxidative decarboxylation. An acute encephalopathy with ketoacidosis characterizes the classic and intermittent forms (see Chapters 1 and 10). The levels of dehydrogenase enzyme activity in the intermediate and intermittent forms are approximately the same (5%40%), whereas activity in the classic form is 0%2% of normal.
Syndromes
- Bleeding or blood pooling where the catheter is inserted
- Your surgeon will make a surgical cut in your groin after using some numbing medicine. You will also be given medicine to relax you.
- Possible weight gain because of slowed metabolism
- Skin rash that looks like fine red spots (petechiae)
- Eosinophils
- Tomato products
- Talwin Nx
Related Products
Usage: q.d.
Additional information:
8 of 10
Votes: 115 votes
Total customer reviews: 115
Customer Reviews
Sigmor, 43 years: Epidural and subdural hematomas are almost impossible to distinguish on clinical grounds alone. Cervicomedullary tumors cause neck discomfort, weakness or numbness of the hands, and an asymmetric quadriparesis.
Lars, 23 years: Hemodialysis reverses the encephalopathy and should be accomplished as quickly as possible after diagnosis. Studies in fetuses and newborn infants with hypoplastic left heart have demonstrated that head circumference is less than normal23 and that cerebral development is impaired.
Contact
0673406227
dppsmyanmar@gmail.com