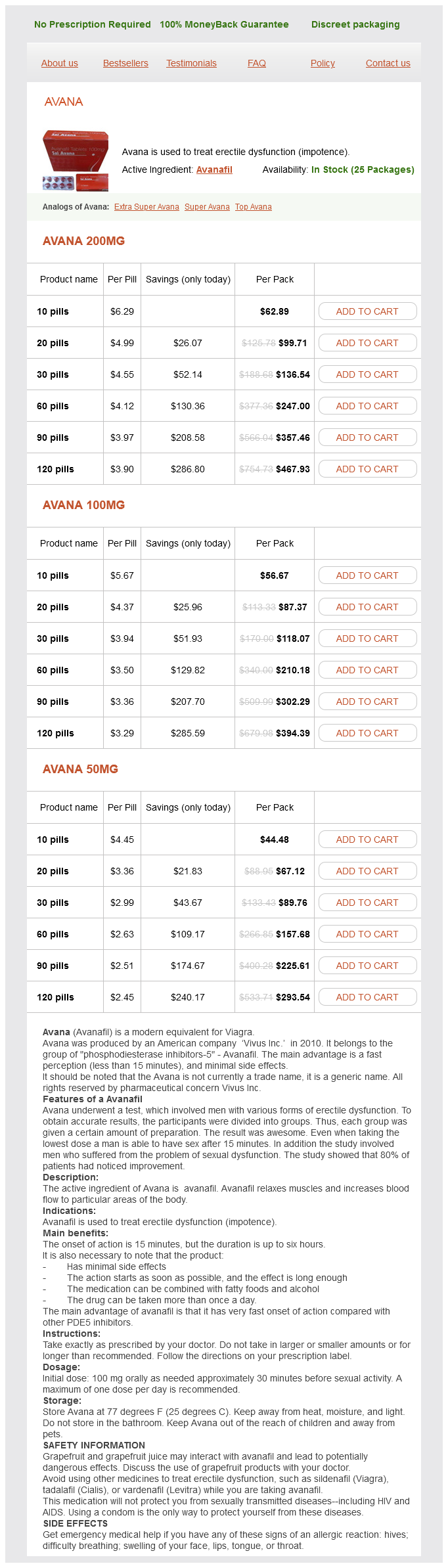
Avana
Avana 200mg
- 10 pills - $62.89
- 20 pills - $99.71
- 30 pills - $136.54
- 60 pills - $247.00
- 90 pills - $357.46
- 120 pills - $467.93
Avana 100mg
- 10 pills - $56.67
- 20 pills - $87.37
- 30 pills - $118.07
- 60 pills - $210.18
- 90 pills - $302.29
- 120 pills - $394.39
Avana 50mg
- 10 pills - $44.48
- 20 pills - $67.12
- 30 pills - $89.76
- 60 pills - $157.68
- 90 pills - $225.61
- 120 pills - $293.54
Avana dosages: 200 mg, 100 mg, 50 mg
Avana packs: 10 pills, 20 pills, 30 pills, 60 pills, 90 pills, 120 pills
In stock: 680
Only $2.6 per item
Description
Failure to do so will lead to the elimination of the unsuccessful B or T cells by programmed cell death (Nemazee erectile dysfunction drugs in ghana purchase avana 50 mg on-line, 2006). These recombination and subsequent somatic hypermutation events are vital for an optimally performing adaptive immune system. Note that protein degradation occurs continuously, even in the absence of infection. These structurally related molecules are expressed on different cell types but perform parallel functions in priming T-cell responses. These receptors rarely, if ever, recognize self-antigens expressed by healthy cells. The goal of lymphocyte development is to produce cells with functional pathogen receptors but eliminate cells whose receptors recognize self-antigens. Next, we describe the processes of B-cell and T-cell development and highlight the mechanisms that maintain self-tolerance. In this pathway, extracellular pathogens are internalized by host cells through endocytosis or phagocytosis and are degraded by proteolytic enzymes within endocytic vesicles. B-cell development can be broadly divided into pro-B-, pre-B-, immature B-, and mature B-cell stages. By the immature B-cell stage, B cells express fully rearranged IgM immunoglobulins on their cell surface. At this stage, immature B cells leave the bone marrow and complete their maturation in the periphery. Mature B cells express both IgM and IgD immunoglobulins on their cell surfaces (LeBien and Tedder, 2008). Consequently, B cells do not undergo as rigorous of a selection process as T cells. However, B cells whose receptors recognize components of the bone marrow are negatively selected and die by apoptosis. T-Cell Development Unlike B cells, which develop in the bone marrow, T-cell precursors complete their development in the thymus. After this period of rapid proliferation, T cells begin to rearrange their -chain genes. Because cells within each clone can rearrange a different chain, they generate a more diverse population than if the original cell had rearranged both the chain and chain before proliferating. After positive selection, T cells migrate to the thymic medulla to undergo negative selection.
Inchinko (Yin Chen). Avana.
- How does Yin Chen work?
- Hepatitis, jaundice, gallstones, high cholesterol levels, increasing bile flow from the gallbladder, hepatitis C infections, fever and chills, bitter taste in the mouth, chest tightness, flank pain, dizziness, nausea, loss of appetite, headache, constipation, painful urination, itching, tumors, joint pain, painful periods, malaria, or spasms.
- Are there safety concerns?
- What is Yin Chen?
- Are there any interactions with medications?
- Dosing considerations for Yin Chen.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96316
Interactions between cyclosporine and sirolimus require that administration of the two drugs be separated by time best erectile dysfunction vacuum pump order avana 100 mg on-line. Sirolimus aggravates cyclosporine-induced renal dysfunction, while cyclosporine increases sirolimus-induced hyperlipidemia and myelosuppression. Clinical indications for cyclosporine are kidney, Antiproliferative and Antimetabolic Drugs Sirolimus Sirolimus (rapamycin) is a macrocyclic lactone produced by Streptomyces hygroscopicus. Cyclosporine usually is combined with other agents, especially glucocorticoids and either azathioprine or mycophenolate, and, most recently, sirolimus. The dose of cyclosporine varies, depending on the organ transplanted and the other drugs used in the specific treatment protocol(s). The initial dose generally is not given before the transplant because of the concern about nephrotoxicity. For renal transplant patients, therapeutic algorithms have been developed to delay cyclosporine or tacrolimus introduction until a threshold renal function has been attained. Dosing is guided by signs of rejection (too low a dose), renal or other toxicity (too high a dose), and close monitoring of blood levels. Great care must be taken to differentiate renal toxicity from rejection in kidney transplant patients. Ultrasound-guided allograft biopsy is the best way to assess the basis for renal dysfunction. Because adverse reactions have been ascribed more frequently to the intravenous formulation, this route of administration is discontinued as soon as the patient can take the drug orally. In rheumatoid arthritis, cyclosporine is used in severe cases that have not responded to methotrexate. Cyclosporine can be combined with methotrexate, but the levels of both drugs must be monitored closely. In psoriasis, cyclosporine is indicated for treatment of adult immunocompetent patients with severe and disabling disease for whom other systemic therapies are contraindicated or have failed. Because of its mechanism of action, there is a theoretical basis for the use of cyclosporine in a variety of other T-cellmediated diseases. A newer indication for sirolimus is the avoidance of calcineurin inhibitors, even when patients are stable, to protect kidney function (Schena et al. The principal adverse reactions to cyclosporine therapy are renal dysfunction and hypertension; tremor, hirsutism, hyperlipidemia, and gum hyperplasia also are frequently encountered. Hypertension occurs in about 50% of renal transplant and almost all cardiac transplant patients. Hyperuricemia may lead to worsening of gout, increased P-glycoprotein activity, and hypercholesterolemia (see Chapters 5, 33, and 38). Nephrotoxicity occurs in the majority of patients and is the reaches a peak blood concentration within about 1 h after a single dose in healthy subjects and within about 2 h after multiple oral doses in renal transplant patients.
Specifications/Details
Therefore erectile dysfunction treatment fruits order 200 mg avana overnight delivery, it is important to monitor the reticulocyte index over the first several weeks. If it does not continue at elevated levels while the hematocrit is below 35%, plasma concentrations of iron and folic acid should again be determined and the patient reevaluated for an illness that could inhibit the response of the marrow. The degree and rate of improvement of neurological signs and symptoms depend on the severity and the duration of the abnormalities. Those that have been present for only a few months usually disappear relatively rapidly. When a defect has been present for many months or years, full return to normal function may never occur. This fact must be impressed on the patient and family, and a system must be established to guarantee continued monthly injections of cyanocobalamin. Intramuscular injection of 100 g of cyanocobalamin every 4 weeks is usually sufficient. Patients with severe neurological symptoms and signs may be treated with larger doses of vitamin B12 in the period immediately after the diagnosis. Doses of 100 g per day or several times per week may be given for several months with the hope of encouraging faster and more complete recovery. It is important to monitor vitamin B12 concentrations in plasma and to obtain peripheral blood counts at intervals of 36 months to confirm the adequacy of therapy. Intranasal preparations are available for maintenance following normalization of vitamin B12deficient patients without nervous system involvement. It is not the principal folate congener in food or the active coenzyme for intracellular metabolism. After absorption, PteGlu is rapidly reduced at the 5, 6, 7, and 8 positions to tetrahydrofolic acid (H4PteGlu), which then acts as an acceptor of a number of one-carbon units. These are attached at either the 5 or the 10 position of the pteridine ring or may bridge these atoms to form a new five-member ring. This reaction requires tetrahydrofolate as an acceptor of a methylene group from serine and uses pyridoxal phosphate as a cofactor. In uncomplicated pernicious anemia, in which the abnormality is restricted to a mild or moderate anemia without leukopenia, thrombocytopenia, or neurological signs or symptoms, the administration of vitamin B12 alone will suffice. In this situation, a therapeutic trial with small amounts of parenteral vitamin B12 (110 g per day) can confirm the presence of an uncomplicated vitamin B12 deficiency. In contrast, patients with neurological changes or severe leukopenia or thrombocytopenia associated with infection or bleeding require emergency treatment. X represents additional residues of glutamate; polyglutamates are the storage and active forms of the vitamin. By these reactions, carbon atoms at positions 8 and 2, respectively, are incorporated into the growing purine ring. This pathway may provide 200 g or more of folate each day for recirculation to tissues.
Syndromes
- Diarrhea
- Have a weak immune system from cancer treatment, certain medicines, or severe wounds
- 5-HIAA
- What other symptoms do you have?
- Eggs
- Guilt
Related Products
Usage: p.o.
Additional information:
8 of 10
Votes: 59 votes
Total customer reviews: 59
Customer Reviews
Sebastian, 62 years: Catecholamines enhance cardiac myocyte automaticity and lower the Other Actions, Good and Adverse.
Olivier, 23 years: Proteomic approaches and identification of novel therapeutic targets for alcoholism.
Contact
0673406227
dppsmyanmar@gmail.com