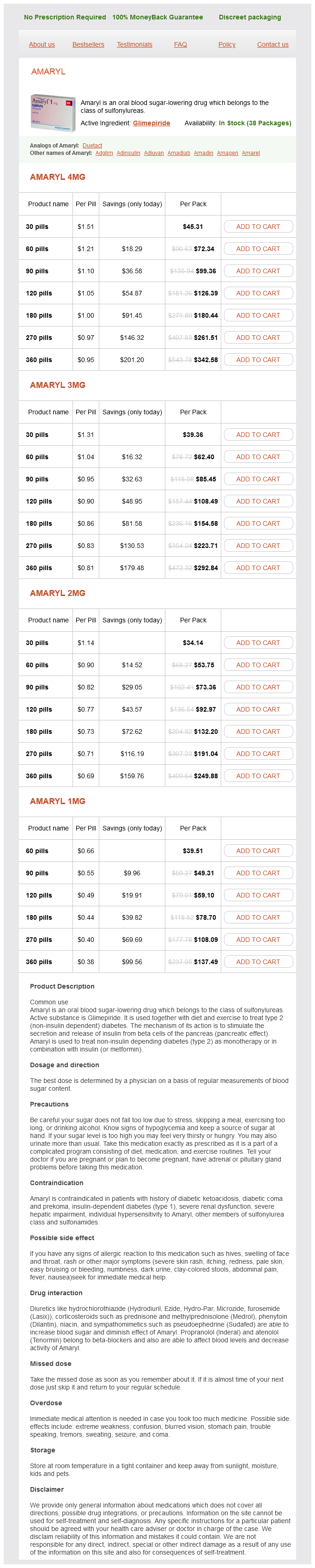
Amaryl
Amaryl 4mg
- 30 pills - $45.31
- 60 pills - $72.34
- 90 pills - $99.36
- 120 pills - $126.39
- 180 pills - $180.44
- 270 pills - $261.51
- 360 pills - $342.58
Amaryl 3mg
- 30 pills - $39.36
- 60 pills - $62.40
- 90 pills - $85.45
- 120 pills - $108.49
- 180 pills - $154.58
- 270 pills - $223.71
- 360 pills - $292.84
Amaryl 2mg
- 30 pills - $34.14
- 60 pills - $53.75
- 90 pills - $73.36
- 120 pills - $92.97
- 180 pills - $132.20
- 270 pills - $191.04
- 360 pills - $249.88
Amaryl 1mg
- 60 pills - $39.51
- 90 pills - $49.31
- 120 pills - $59.10
- 180 pills - $78.70
- 270 pills - $108.09
- 360 pills - $137.49
Amaryl dosages: 4 mg, 2 mg, 1 mg
Amaryl packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 997
Only $0.41 per item
Description
Most hypokinetic diabetes and depression buy amaryl 1 mg fast delivery, hyperkinetic, and ataxic movement disorders will slowly worsen over time. Disorders that improve over time are less common; for example, tic disorders will typically improve from childhood into adolescence and adulthood. Although many movement disorders start out as intermittent or suppressible, they tend to become more continuous or constant when they progress over time. The rest tremor seen in parkinsonian disorders is a classic example, where the tremor starts intermittently in a limb before becoming more regular and spreading to other limbs. Early on, this type of tremor can be sometimes voluntarily suppressed or decreased with movement, but later the tremor is continuous. Paroxysmal disorders, which are typically choreic or dystonic in nature, can many times be diagnosed by history alone if specific triggers such as sudden movements cause the disorder to occur. For example, restless legs syndrome worsens at night when the patient is laying down. All modes of inheritance patterns are seen in movement disorders and the genetic basis of these disorders is rapidly being discovered. It is not sufficient to inquire only about the particular movement disorder seen in the patient, since broadening the questioning to other biological family members may yield additional important clues. For example, patients with grandchildren with intellectual disabilities may be at risk for fragile X-associated disorders. Tic patients may have associated diagnoses in the family, such as attention deficit hyperactivity disorder. The majority of movement disorders are restricted to the nervous system, but systemic organ involvement may provide diagnostic clues. For example, patients with underlying cancers may be at risk for paraneoplastic disorders and iron deficiency anemia or diabetes may predispose to restless legs syndrome. The presence of cardiomyopathy is associated with Friedreich ataxia or mitochondrial disorders. Enlargement of visceral organs (spleen, liver) may suggest a lysosomal storage disease. Have the movements been treated in the past and what was the response to treatment A response to dopamine medications may facilitate diagnosis of doparesponse dystonia. Paroxysmal movement disorders may be exquisitely responsive to antiepileptic medications. Other substances may improve movements, such as the improvement Approach to Movement Disorders 3 of essential tremor, essential myoclonus, and myoclonusdystonia with alcohol.
Psoralea tetragonoloba (Guar Gum). Amaryl.
- Are there any interactions with medications?
- How does Guar Gum work?
- Diabetes.
- What other names is Guar Gum known by?
- Are there safety concerns?
- High cholesterol.
- Constipation.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96883
The pie slice organization of the brainstem does not simply distinguish between motor and sensory diabetes video cheap amaryl 4 mg with mastercard. Instead, there are characteristic locations for subtypes of motor and sensory functions. The subcategory of branchial motor refers to muscles derived from branchial arches, also known as pharyngeal arches, which are transient developmental structures of the vertebrate embryo that give rise to some but not all of the muscles in the head. The remaining muscles of the head, along with muscles of the body, derive from somites. In fish, branchial arches develop into the gills; in mammals, they complement rostral somites to become the source of bones, cartilage, and muscles in the head region. Muscles arising from branchial arches are termed branchiomeric muscles, and the motoneurons that innervate them are branchial motoneurons. There are no known differences in the functional properties of adult branchiomeric and somite-driven muscles. Nonetheless, the distinction is helpful to learning the anatomy of cranial nerve nuclei and exit points. Additionally, learning the terms enables you to read the human and nonhuman research literature. The term skeletomotor will be used to refer to all skeletal muscles, including both branchiomeric and somatic motor (referred to as somatomotor here) ones. The oculomotor nerves exit from the medial margin of the cerebral peduncles (cp) that mark the midbrain ventrum. Diencephalic structures include the mammillary bodies (mb), infundibular stalk (is), optic tract and chiasm (ox), lateral geniculate body (lgb), and thalamus. Within each pie slice, subtypes of sensory and motor functions occupy specific regions. The most medial region of the medial motor pie slice contains somatic motoneurons. Lateral to this most medial region, but still medial to the sulcus limitans, visceromotor neurons. Pie slices lateral to the sulcus limitans contain secondary sensory neurons that receive input from visceral afferents and taste inputs medially and somatosensory and special afferents more laterally. For the purposes of cranial nerve exits, considering four slices of the brainstem suffices. A magnified view, shown at right, shows the exit of the trochlear nerve near the junction between the pons and midbrain, just caudal to the inferior colliculus (ic), an auditory processing region in the caudal midbrain.
Specifications/Details
In addition diabetes mellitus medline amaryl 4 mg with amex, both of these disorders have neuromuscular involvement and might have hepatosplenomegaly, which can help narrow the differential. In ChAc, the motor phenotype includes limb and orolingual dystonia including the characteristic "feeding dystonia," where the tongue protrudes and pushes food out of the mouth. In addition, there may be prominent selfmutilation in the form of tongue biting and lipbiting. Seizures may be the first manifestation of the disease, and psychiatric manifestations including psychosis and obsessivecompulsive behaviors are also common. Psychosis, obsessivecompulsive disorder, and depression are common, and may predate the movement abnormalities. There is prominent myopathy with muscle atrophy, and cardiomyopathy with conduction abnormalities and life threatening arrhythmias can occur. Onset of neurological symptoms is in the first decade, with orofacial and limb dystonia, spasticity, and chorea. Lingual dystonias, including the feeding dystonia seen with ChAc, may respond to some degree to botulinum toxin injections in the genioglossus. Anticonvulsants, such as valproate, used to treat seizures may help the involuntary movements as well. Supportive care, including speech therapy, to help with dysphagia and physical/ occupational therapies to improve gait impairment are generally required. Acquired choreas Chorea may also present as a symptom of metabolic and endocrine disorders, vascular disorders (including inflammatory vasculitides), infectious or parainfectious processes, and toxicity related to medications or other agents (Table 6. For many acquired choreas, removal of the inciting cause may help alleviate chorea. When the cause is a structural lesion, the abnormal movements generally improve with time, although symptomatic treatment may be helpful in the acute stages or with disabling movements. Behavioral and psychiatric abnormalities 54 Non-Parkinsonian Movement Disorders Box 6. Other features of acute rheumatic fever, such as carditis and arthritis, may also be present. There may be discordance between the extent of psychiatric and neurological involvement. Patients should also be advised to seek primary treatment for future streptococcal pharyngitis. Other than elimination of the streptococcal infection, the major principles of management include symptomatic treatment of abnormal movements and behavioral and psychiatric features, in addition to treating the inflammatory/immune response. Typical neuroleptics like haloperidol control chorea effectively but are commonly associated with adverse effects including druginduced parkinsonism.
Syndromes
- Deep vein thrombosis (blood clots that form when someone is inactive or confined to bed)
- Zinc: Sources of this mineral include beans and foods fortified with zinc, such as milk and cereals.
- Muscle spasms
- Renal disease (See: kidney failure)
- Difficulty walking (ataxia)
- Pain, usually in the upper right part of the abdomen
- Infection
- Lump on thyroid gland
- Digoxin: greater than 2.4 ng/mL
Related Products
Usage: p.r.n.
Additional information:
8 of 10
Votes: 92 votes
Total customer reviews: 92
Customer Reviews
Roy, 49 years: A progressive dementia develops, with memory loss and eventually a nearly total loss of cognition.
Silas, 53 years: When the stapedius is contracted, the stapes cannot hit the oval window as forcefully, and this reduces the amount of pressure that is communicated to the cochlea.
Contact
0673406227
dppsmyanmar@gmail.com