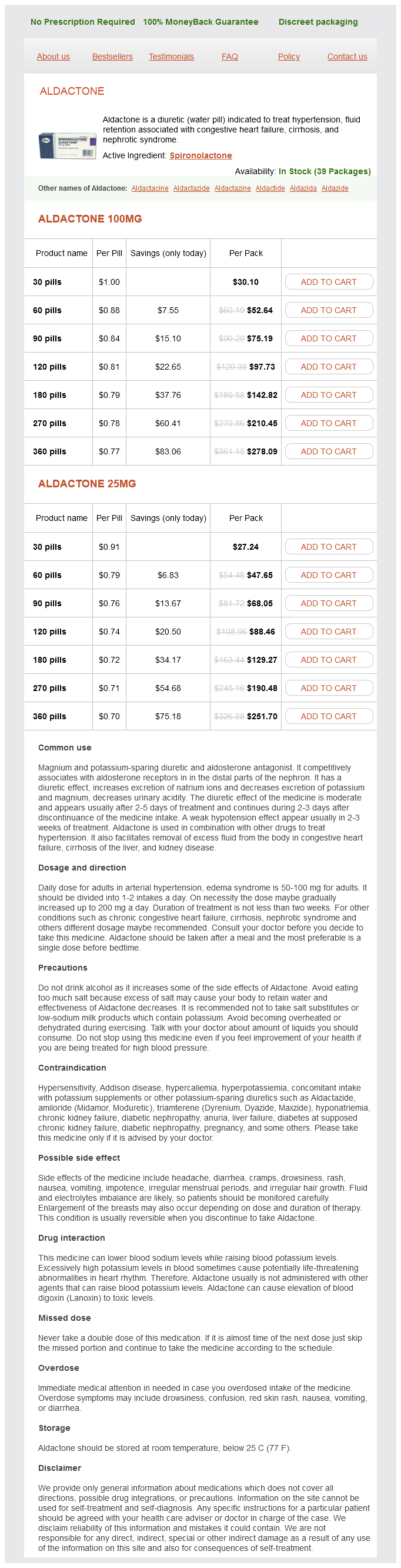
Aldactone
Aldactone 100mg
- 30 pills - $30.10
- 60 pills - $52.64
- 90 pills - $75.19
- 120 pills - $97.73
- 180 pills - $142.82
- 270 pills - $210.45
- 360 pills - $278.09
Aldactone 25mg
- 30 pills - $27.24
- 60 pills - $47.65
- 90 pills - $68.05
- 120 pills - $88.46
- 180 pills - $129.27
- 270 pills - $190.48
- 360 pills - $251.70
Aldactone dosages: 100 mg, 25 mg
Aldactone packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 908
Only $0.62 per item
Description
For early-stage oral tongue cancer blood pressure pills buy aldactone 100 mg, depth of invasion and worst pattern of invasion are the strongest pathological predictors for locoregional recurrence and mortality. Randomized trial addressing risk features and time factors of surgery plus radiotherapy in advanced head-and-neck cancer. Combined postoperative radiotherapy and weekly cisplatin infusion for locally advanced head and neck carcinoma: Final report of a randomized trial. Stereotactic body radiotherapy for recurrent head and neck cancer: A critical review. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. Radiotherapy plus cetuximab for locoregionally advanced head and neck cancer: 5-year survival data from a phase 3 randomised trial, and relation between cetuximab-induced rash and survival. Hyperfractionated or accelerated radiotherapy in head and neck cancer: A meta-analysis. Results of a prospective trial on elective modified radical classical versus supraomohyoid neck dissection in the management of oral squamous carcinoma. Hyperfractionated irradiation with or without concurrent chemotherapy for locally advanced head and neck cancer. Patterns of failure, prognostic factors and survival in locoregionally advanced head and neck cancer treated with concomitant chemoradiotherapy: A 9-year, 337-patient, multi-institutional experience. Occult metastases detected by sentinel node biopsy in patients with early oral and oropharyngeal squamous cell carcinomas: Impact on survival. A meta-analysis of hyperfractionated and accelerated radiotherapy and combined chemotherapy and radiotherapy regimens in unresected locally advanced squamous cell carcinoma of the head and neck. Frequency and therapeutic implications of "skip metastases" in the neck from squamous carcinoma of the oral tongue. Randomized trial of radiation therapy versus concomitant chemotherapy and radiation therapy for advanced-stage oropharynx carcinoma. Verrucous carcinoma of the oral mucosa: An epidemiological and follow-up study of patients treated with surgery in 5 last years. Elective neck dissection in early-stage oral squamous cell carcinomadDoes it influence recurrence and survival Dosimetric factors associated with long-term dysphagia after definitive radiotherapy for squamous cell carcinoma of the head and neck. Prognostic impact of marginal mandibulectomy in the presence of superficial bone invasion and the nononcologic outcome. Osteoradionecrosis of mandible bone in patients with oral cancer-associated factors and treatment outcomes. Prior chemoradiotherapy adversely impacts outcomes of recurrent and second primary head and neck cancer treated with concurrent chemotherapy and reirradiation. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. Causes of cancer in the world: Comparative risk assessment of nine behavioural and environmental risk factors.
Klapperschlangen (Senega). Aldactone.
- Are there safety concerns?
- How does Senega work?
- Asthma; emphysema; bronchitis; swelling (inflammation) of the throat, nose, and chest; and other conditions.
- Dosing considerations for Senega.
- What is Senega?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96668
Differentiating between disease subtypes is made based on immunophenotyping by flow cytometry and/or immunohistochemistry hypertension 4019 order 100 mg aldactone free shipping. Complementary cytogenetic or molecular analyses to detect characteristic chromosomal translocations or genetic alterations, or to establish clonality, may also be necessary in some cases. For detailed information on cell surface and genetic markers as well as on staging and risk stratification, refer to the entry in the "Pathology and Genetics" section. In particular, the management strategies are very different between those for indolent (low-grade) and those for aggressive (high-grade) disease. Observation is also common practice for patients with advanced but low tumor burden disease. Surgical resection may additionally be considered in symptomatic localized disease. Since the introduction of rituximab, single-agent systemic therapy with chlorambucil or cyclophosphamide, or with the purine analogs fludarabine and cladribine, is used increasingly less frequently but can still be effective in some patients. Antibody monotherapy with rituximab or using radio-immunoconjugates, like ibritumomab tiuxetan (ZevalinÒ), or treatment with chlorambucil plus rituximab, remain alternatives for lower risk patients or when conventional chemotherapy is contraindicated. Rituximab or radioimmunotherapy are recommended for consideration as maintenance therapy following the combined rituximab/chemotherapy regimen in patients with high-burden tumors. Therefore, this approach is not recommended as the first-line therapy of responding patients. Multiple options exist for the treatment of patients who relapse or progress after the first-line therapy. Fludarabine-based regimens are another option for patients who relapse after an alkylator-based therapy. However, they may not be suitable for heavily pretreated elderly patients in whom rituximab (in case of rituximab-sensitive disease) or radioimmunotherapy may be better options. Still, most patients eventually relapse and there is an increased rate of secondary malignancies. Therefore, this option is only recommended for young patients with adverse presentations, including early relapse after first-line treatment. Second-line chemotherapy regimens often employ high-dose cytosine arabinoside or gemcitabine, corticosteroids, and platinum-containing chemotherapeutic agents with or without etoposide. Any of these regimens could be combined with rituximab if the patient is deemed to be responsive to this agent. Thus, by mutating multiple genes, and by favoring chromosomal translocations, aberrant hypermutation may represent a major contributor to lymphomagenesis. The presence of intraclonal variation within lymphoid neoplasms is taken as indicative of ongoing mutations, and therefore a relationship to the germinal center. Definition and Principles of Classification Lymphoid neoplasms represent a large group of clonal proliferations derived from immature or mature lymphoid cells. They encompass a variety of distinct diseases with different clinical presentations, pathological features and biological behavior.
Specifications/Details
The surrounding tissue often shows obstructive changes with fibrosis and acinar cell atrophy blood pressure medication plendil buy 100 mg aldactone free shipping. All these aspects contribute to explain the high frequency of microscopically incomplete resections (R1-resections) that are encountered also in high-volume centers if pancreatic resection specimens are carefully analyzed according to standardized procedures. This is based on studies showing a significant impact on prognosis of the number of affected lymph nodes. In addition to the presence of lymph node metastases and their number, the ratio between affected lymph nodes to the total number of retrieved lymph nodes (so-called lymph node ratio) has been shown to significantly impact on prognosis as well. Distant metastases are commonly found in the liver (65%), lungs, and more rarely in bones or adrenals. Local tumor recurrences and/or distant metastases occur in the first 2 years after resection in about 70% of patients. However, about half of the cases show heterogeneous differentiation with additional growth components. Well or poorly differentiated (G1 or G3) tumors are reported in 10%30% of the cases. These include the adenosquamous carcinoma, characterized by solid-squamous differentiation, the mucinous (colloid) carcinoma, characterized by the presence of abundant extracellular mucin, the rare signet-ring cell carcinoma, the large-duct type adenocarcinoma, characterized by the presence of well-differentiated, large ductal structures, the medullary carcinoma, the hepatoid carcinoma, the undifferentiated (anaplastic) carcinoma and the undifferentiated carcinoma with osteoclastic-like giant cells. An impact on survival depending on variant type has been described, with the adenosquamous and undifferentiated variants bearing the worst prognosis. Multinodular growth, as well as the presence of areas of necrosis and hemorrhage, have been described. A cystic variant, which may reach a very large size (> 20 cm), and an intraductal variant with papillary growth have been reported. Grossly, tubulo-papillary carcinomas form a solid whitish mass with pushing borders. Histologically, they consist of back-to-back tubules or glands as well as papillary structures without overt mucin production. Tubulo-papillary carcinomas are reminiscent of acinar cell or even neuroendocrine neoplasms, and immunohistochemistry may be useful to make the diagnosis. Carcinomas with mixed differentiation Carcinomas with mixed acinar-ductal, ductal-neuroendocrine, acinar-neuroendocrine and even acinar-ductal-neuroendocrine features have been reported. Each component should be detected in at least one-third of the tumor mass to warrant a diagnosis of mixed neoplasm. These subtypes are distinguished on the basis of their growth pattern and proliferative activity, assessed by mitotic count or preferably by the Ki-67 index. The different key genetic events involved in these two entities support this concept. Distant metastases occur late and may affect different organs, such as liver, lung and bone. The cells are monotonous and often display granular cytoplasm and granular chromatin, known as "salt and pepper" chromatin. Stage and grade have emerged as the most potent predictive factors in most studies.
Syndromes
- Cloudy or bloody urine, which may have a foul or strong odor
- Use of alcohol or other recreational drugs
- Abnormal sound, called a murmur, when a stethoscope is placed over the abnormal blood vessel
- Skin rash
- If you are nursing, the doctor will probably recommend that you continue nursing. Breast-feeding helps prevent diarrhea, and it also speeds recovery.
- In the back of the middle of the head (posterior fontanelle)
- Procedures to reduce feeling in the nerve (such as nerve ablation using radiofrequency, heat, balloon compression, or injection of chemicals)
- Is it present all of the time or only sometimes?
- Aspirin-containing compounds
- Inguinal hernia appears as a bulge in the groin or scrotum. This type is more common in men than women.
Related Products
Usage: gtt.
Additional information:
8 of 10
Votes: 237 votes
Total customer reviews: 237
Customer Reviews
Aila, 43 years: The second echelon draining lymphatics for both lips are the upper anterior cervical nodes, though occasionally direct spread may occur. The coronal image shows inferior extension into the floor of mouth/sublingual space (solid white arrow in B) and medial involvement of the genioglossus muscle. A bone scan is indicated in patients with bone pain and/or elevated alkaline phosphatase levels.
Mason, 46 years: The list of tumors in the colon therefore does contain, in addition to adenocarcinomas, also fibromas, leiomyomas, gastrointestinal stromal tumors (derived from the interstitial cells of Cajal, the pacemakers of intestinal peristaltic movement), lipomas, neurofibromas, ganglioneuromas, and lymphomas. Several retrospective analyses have suggested that diabetics treated with metformin during chemotherapy have longer survival than individuals treated with other antidiabetic agents. Neither were intended to serve as a basis for clinical decisions in routine oncology, and indeed they are too rigid for this purpose.
Contact
0673406227
dppsmyanmar@gmail.com