Adalat
Adalat 30mg
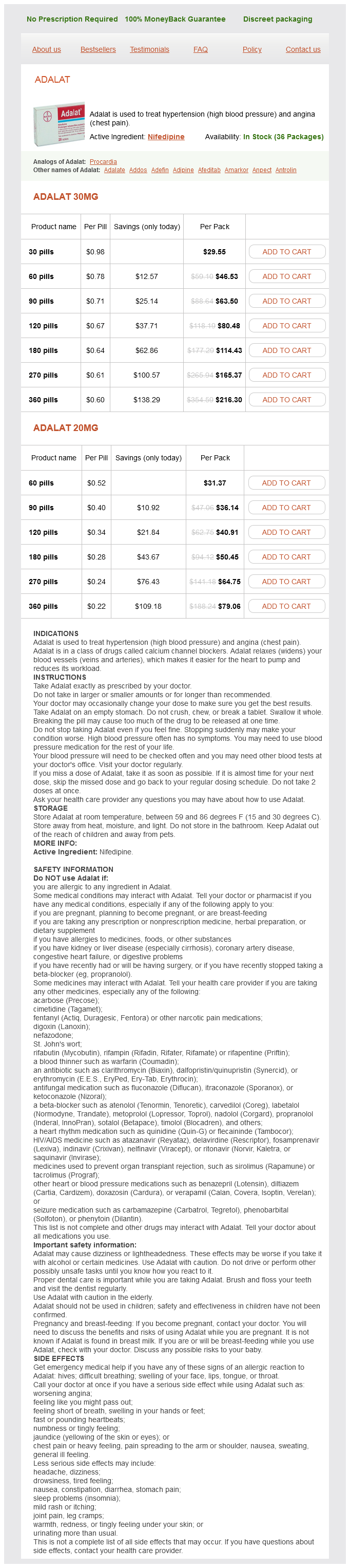
- 30 pills - $29.55
- 60 pills - $46.53
- 90 pills - $63.50
- 120 pills - $80.48
- 180 pills - $114.43
- 270 pills - $165.37
- 360 pills - $216.30
Adalat 20mg
- 60 pills - $31.37
- 90 pills - $36.14
- 120 pills - $40.91
- 180 pills - $50.45
- 270 pills - $64.75
- 360 pills - $79.06
Adalat dosages: 30 mg, 20 mg
Adalat packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 728
Only $0.23 per item
Description
In addition arrhythmia and palpitations buy adalat 30 mg low price, it immobilizes the elbow, which is desirable for the first few days after a distal forearm fracture. Construct and apply this splint in the same manner as the forearm portion of the double sugar-tong splint described earlier. Volar Splint A Application B Indications Triquetral fracture A, Begin the splint in the palm at the metacarpal heads and extend it along the volar surface of the forearm to a point just proximal to the elbow. If any of the fingers are injured, extend the splint to incorporate the involved digits. Place the forearm in the neutral (thumb-up) position with the wrist slightly extended (10° to 20°). B, For more serious injuries, add an additional dorsal slab to create a bivalve splint. Soft tissue injuries of the hand and wrist Orthopedic injuries of the hand and wrist, including: Triquetral fractures (shown above) Lunate and perilunate dislocations Second through fifth metacarpal head fractures Minimally displaced distal radius and ulna fractures the volar splint does not eliminate supination and pronation of the forearm and therefore is not ideal for more complicated distal radius and ulna fractures. Keep the elbow flexed at a 90° angle, the forearm in the neutral (thumb-up) position, and the wrist in a neutral position or slightly extended (10° to 20°). Indications Distal radius and ulna fractures (shown above) Distal forearm fractures the forearm sugar-tong splint, unlike the volar wrist splint, prevents supination and pronation of the forearm. Additionally, it immobilizes the elbow, which is desirable for the first few days after a distal forearm fracture. Traditionally, a thumb spica splint or cast was thought to be a requirement for properly immobilizing scaphoid fractures; however, there is no totally agreed standard. Clay and coworkers16 stated that the optimal method of casting scaphoid fractures has not been definitively established. They were unable to prove a difference in patient comfort, recovery of function, or incidence of nonunion between a Colles cast and a traditional scaphoid cast that included the thumb. Because some scaphoid fractures heal poorly under the best of circumstances, it seems prudent to provide thumb immobilization in the initial splinting. Failure to do so, such as when a "sprained wrist" is suspected, should not be construed as being beneath the accepted standard of care. Most volar splints will at least partly immobilize the base of the thumb, so the discussion may be moot. Extend the splint from just distal to the interphalangeal joint of the thumb to the midforearm level. Instead, cut a hole in the stockinette to expose the thumb, and then pad the exposed thumb with small vertical strips of Webril or wrap it with 2-inch Webril.
Medicago (Alfalfa). Adalat.
- What other names is Alfalfa known by?
- How does Alfalfa work?
- Dosing considerations for Alfalfa.
- Are there safety concerns?
- Are there any interactions with medications?
- Kidney, bladder, and prostate problems; asthma; arthritis; diabetes; indigestion; and other conditions.
- Is Alfalfa effective?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96069
Similarly whats prehypertension mean 30 mg adalat overnight delivery, superior dislocation of the patella may be mistaken for high riding patella typical of patellar tendon rupture. Unlike anterior shoulder dislocations, which are often easily detected on plain films, posterior shoulder dislocations may be missed on initial radiographs. A careful history will uncover these injuries and prompt the necessary assessment of the ligamentous integrity and the possibility of an associated vascular injury and guide proper immobilization and follow-up care. Other dislocations that are commonly first seen in a reduced state include finger dislocations, patellar dislocations, and radial head subluxations. Frequently, the initial pain of the dislocation is distracting, and paresthesias or a weak pulse may not be readily apparent until the joint has been reduced. Reasons include difficulty distinguishing a fracture-dislocation by clinical examination and the potential for medicolegal problems if the fracture is not identified before attempts at reduction. More importantly, certain associated fractures predict a poor outcome with closed reduction and make orthopedic consultation a consideration before such attempts. They life-threatening in department can range from a simple finger joint to limb- or consequences of high-energy trauma. Keys to clinical assessment and radiographic evaluation of these injuries are discussed along with methods of reduction. Fracture-dislocations that commonly require operative intervention and emergency orthopedic consultation are not discussed. Each patient and each dislocation is unique, and the treating clinician must use judgment regarding whether premedication is required, which agent or agents to use, and what dose to give. A calm, cooperative patient may tolerate attempts at gentle reduction of a major joint such as the shoulder, but even the most stoic of patients may be quite uncomfortable with the manipulations necessary for reduction of a dislocated finger. A radial head dislocation in a child is usually easily treated without analgesia; however, reduction of a hip dislocation is unlikely to be successful without a significant amount of sedation and analgesia. Attempting any reduction technique in an extremely anxious patient without premedication will generally frustrate the operator and further upset the patient and may hinder a successful outcome. When multiple attempts are required and significant force must be exerted because of muscle spasm or an uncooperative patient, there is an additional chance of producing complications during the reduction. Verbal techniques for alleviating anxiety and discomfort are not to be discounted because they can be of great assistance during joint reduction. In field settings, simple hypnosis techniques have been used successfully for major joint dislocations. Additionally, the use of handheld tablets has shown to aide a variety of painful procedures in the pediatric population and may be a useful adjunct. Standard techniques to assess vascular injury are the strength of the pulse and capillary refill; this should detect most arterial injuries.
Specifications/Details
Other studies have demonstrated elevated tissue interface pressure in patients on spine boards without air mattress padding heart attack vol 1 pt 15 discount adalat 30 mg free shipping. Excessive strapping can interfere with respiratory function in both children73 and adults. Although this may not be a problem in healthy volunteers, the effects on patients with chest trauma or preexisting respiratory disease may be significant. If vomiting does occur, logroll the patient and board as a unit and suction the airway as needed. Although this procedure may be associated with some spinal movement, airway protection takes priority. Conclusion Although spinal immobilization has not been shown to decrease the likelihood of spinal injury and is associated with a variety of complications, prehospital spinal immobilization remains commonplace. Nevertheless, recent evidence supports a widespread shift to selective spinal immobilization by prehospital providers. Until these new recommendations become universal, emergency medicine practitioners should know when spinal immobilization is indicated, recognize properly and improperly applied devices, minimize unnecessary immobilization time, and work with prehospital providers to ensure appropriate indications and proper use. In 1903 archaeologists from the Hearst expedition discovered two specimens whose open fractures had been treated with wooden splints and bandages. Carefully applied splints decrease pain while minimizing further damage to muscles, nerves, and blood vessels. Over the last 3 decades, prehospital splinting materials, equipment, and techniques have evolved considerably. Indications and Contraindications Indications for splinting an extremity are usually clear. Pain after trauma, with or without deformity, should arouse suspicion of underlying bone or joint injury. Other signs include swelling, discoloration, deformity, crepitus, and loss of neurovascular function. However, absence of these findings does not rule out an underlying fracture or dislocation. Thus, in most cases where a musculoskeletal injury is suspected, a splint should be applied and maintained. There are no absolute contraindications to splinting suspected extremity fractures or dislocations. However, in the setting of multisystem trauma with life-threatening injuries, rapid transport may be more important than extremity splinting. Equipment Various types of splints are currently available for immobilizing upper extremity injuries. Emergency care providers should be well trained and familiar with their equipment. Bent into any of three simple curves, it is extremely strong and provides support for any fractured or injured extremity. In addition, it is water resistant, lightweight, radiolucent, reusable, and not affected by extreme temperatures or altitudes.
Syndromes
- Sleep in a curled-up, fetal position with a pillow between your legs. If you usually sleep on your back, place a pillow or rolled towel under your knees to relieve pressure.
- Bleeding
- Amount swallowed
- Delirium or confusion
- Bleeding
- Going down stairs
- Pain or tenderness in the pelvis, lower abdomen, or sometimes the lower back
- Increased chance of urinary tract infection and bowel problems
- Bladder outlet obstruction - blockage of the bladder that does not allow drainage
- Blood alcohol level
Related Products
Usage: q._h.
Additional information:
8 of 10
Votes: 220 votes
Total customer reviews: 220
Customer Reviews
Georg, 48 years: Because outpatient management of burns should be attempted only when the risk for infection is minimal, the use of systemic antibiotics is unnecessary for minor burns, even in the setting of delayed treatment, diabetes, and steroid use. The block could be unsuccessful if the needle insertion is too superficial for the anesthetic to reach the nerve. After reduction, send the child home with a pressure dressing and stool softeners.
Kurt, 31 years: Protect the needle from accidental dislodgement by cutting the bottom out of a plastic cup and taping and bandaging the cup in place over the device. Stahl S, kaufman T: the efficacy of an injection of steroid for medial epicondylitis: a prospective study of sixty elbows. Avoid continuous suction because it may attract bowel or omentum to the end of the paracentesis needle with resultant occlusion.
Contact
0673406227
dppsmyanmar@gmail.com